Transcription
RNSTAFFINGRATIOSA Necessary Solution tothe Patient Safety Crisisin U.S. HospitalsOur Patients. Our Union. Our Voice.
RN STAFFING RATIOS ARESAVING LIVES AND BRINGINGRNs BACK TO THE BEDSIDENNU stands ready to help you bringratios to your stateDear colleague,To be a nurse is to care for people in their mostvulnerable moments, to bring comfort to those inpain, and to bring hope and compassion to thosewho feel hopeless or forgotten. To be a nurse isto watch for subtle changes and to attend to tinydetails. It is a job that requires endless stamina, aniron will, and the time to get it right. As registerednurses who work at the bedside, we know theimportance of attending to the needs of a sickchild, a frightened cancer patient, or a patient inthe throes of a mental health crisis. We also knowthe pain of feeling you don’t have the support youneed to provide the care that your patients need.With all the cutbacks, we know that the solutionlies in our fight back.NNU’s proposal for minimum, mandated, nurseto-patient staffing ratios protect our patients’right to nursing care. We know that every patientdeserves a single standard of high-quality care.The ratios, coupled with nurses’ powerful voice ofadvocacy secured in collective bargaining, protectour patients from complications that arise frommissed care such as medical errors, health caredisparities, infections, and so much more. We havealso learned from the California experience thatthe pathway to winning lies in building a powerfulorganization where nurses have the right toadvocate to their fullest potential.Currently, California is the only state to enactan RN-to-patient staffing law, thanks to thedetermined, multi-year efforts of members of theCalifornia Nurses Association (CNA). Since thelaw went into effect in all California acute-carehospitals in 2004, nurses have come back to thebedside to provide patient care that more fullyreflects the art and science that our profession isfounded upon.1CNA was the author, sponsor, and driving forcebehind the landmark law, which was signed in1999. The hospital industry and its allies have triedrepeatedly to overturn or weaken the law, but CNAmembers continue to successfully defend ratios.When CNA founded National Nurses OrganizingCommittee (NNOC) in 2005 to represent andadvocate for nurses outside of California, NNOCcontinued the fight to expand the protections ofratios across the nation. Today, CNA/NNOC andthe national nursing union it belongs to, NationalNurses United, fight to pass ratios laws at both thestate and federal level.A seminal 2010 University of Pennsylvania studyshowed that the California law saves thousandsof patient lives, and that if California’s 1:5 ratioswere matched, surgical units in New Jerseyhospitals would have 14 percent fewer deathsand Pennsylvania 11 percent fewer deaths.Consequently, we worked with NNU membersacross the nation and with federal legislatorsto introduce bills that would make these samelifesaving protections the law from coast to coast.As elected leaders of NNU, we are proud to standside by side with nurses across the nation whohave been inspired to rise up together and demandthe best care for their patients by joining withNNU to have the right to fight for ratios throughcollective bargaining. We have watched withgreat hope as nurses from coast to coast build amovement for safe staffing starting in their ownfacilities and continuing on to our nation’s capital.As the authority on nurse-to-patient ratios,NNU is poised to broaden the victories won byCalifornia nurses and patients. Now is the timefor every nurse to become a part of the NATIONALMOVEMENT FOR SAFE STAFFING! Visit ourwebsite at www.NationalNursesUnited.org tobecome a part of our efforts to win mandatedRN-to-patient ratios in every state and forevery patient.Deborah Burger, RN; Jean Ross, RN;Zenei Triunfo-Cortez, RNCouncil of Presidents, NNU2
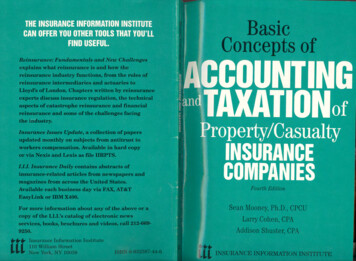
RN RATIOS 101Ratios 101 California’s Safe Staffing Ratios Law— It’s more than just the numbersCalifornia’s historic first-in-the-nation safestaffing ratios, sponsored by CNA, have beenin effect since January 2004 despite continuedefforts of the hospital industry to overturnthe law.The bill was enacted in 1999 following anextensive grassroots campaign by RNs withbroad support from patients and the generalpublic that included thousands of letters, calls,and a massive CNA rally on the steps of the stateCapitol in Sacramento on the day of the finallegislative vote. A concurrent public opinion pollfound that 77 percent of Californians believed itis “a good idea to have a certain safe number oftrained registered nurses per patient to protectthe quality of care” and 69 percent “wouldexpect” the governor to sign the bill. Shortlyafter, Gov. Gray Davis signed the bill into law.Hospital executives lobbied to defeat the law,tried to persuade state health officials to adoptunsafely high ratios, filed a lawsuit to try to blockenforcement of the ratios at all times, encouragedhospital managers to evade the letter and spirit ofthe law, and recruited compliant allies to proposemeasures to overturn it. All those efforts havefailed, thanks to the determination of California’snurses to defend safe patient care.Safe RN ratios have improved quality of careand nurse recruitment and retention in Californiahospitals. A recent Texas Center for NursingWorkforce study on hospital nurse staffingvacancy and turnover rates for registered nursesshowed RN turnover rates in California to bedramatically lower than states without ratios,such as Florida and Texas (Texas Center for3Nursing Workforce Studies, 2016). Accordingto Price waterhouse Coopers in its report,“What Works: Healing the Healthcare StaffingShortage”, the cost of replacing one registerednurse is between 40,000– 85,000; given this,it is evident that ratios implementation savesindividual hospitals from both the expenseand clinical disruption of a rapid turnover of itsnursing staff.CALIFORNIA RATIOSStaffing is based on individual patient acuity ofwhich the mandated ratio is the minimumOperating RoomTrauma Patient in ERIntensive/Critical CareNeonatal Intensive CarePost-anesthesia RecoveryLabor & Delivery ICU Patient in ERStep DownAntepartum Postpartum CoupletsPediatrics Emergency RoomTelemetry Other Specialty CareA.B. 394 — the CNA-sponsored safe staffing law — has multiple provisions designed to remedy unsafestaffing in acute-care facilities. California’s safe staffing standards are based on individual patientacuity, of which the RN ratios is the minimum.MANDATES MINIMUM, SPECIFIC,NUMERICAL RATIOSRESTRICTS UNSAFE “FLOATING”OF NURSING STAFFEstablishes minimum, specific, numerical RN-topatient ratios for acute-care, acute-psychiatric, and specialty hospitals.Requires orientation and validated currentcompetence before assigning a nurse to a clinicalarea. Temporary personnel must receive thesame orientation and competency determinationas permanent staff.REQUIRES A PATIENT CLASSIFICATIONSYSTEM — ADDITIONAL RNS ADDEDBASED ON PATIENT ACUITY AND NEEDAPPLIES AT ALL TIMESAdditional RNs must be added to the minimumratios based upon a documented patientclassification system that measures patient needsand nursing care, including severity of illness,complexity of clinical judgment, and the need forspecialized technology.The ratios apply “at all times,” including mealsand breaks, and excused absenc es.REGULATES USE OF UNLICENSED STAFFBARS CUTS IN ANCILLARY STAFFAS A RESULT OF RATIOSHospitals may not assign unlicensed assistivepersonnel to perform nursing functions orperform RN functions under the supervision ofan RN including administration of medication,venipuncture, and invasive procedures protectingRN scope of practice and patient safety.PROHIBITS AVERAGINGThere can be no averaging of the number ofpatients and the total number of RNs.In the first year of implementation, CNAsuccessfully fought off challenges from severalCalifornia hospitals who responded to the ratiosby attempting to cut back on LVNs and unlicensedpersonnel, going against the intent of the law.The state’s safe staffing standards maintain theexisting staffing model which utilizes RNs, LVNs, and unlicensed assistive personnel.Medical/SurgicalPostpartum Women OnlyPsychiatric4
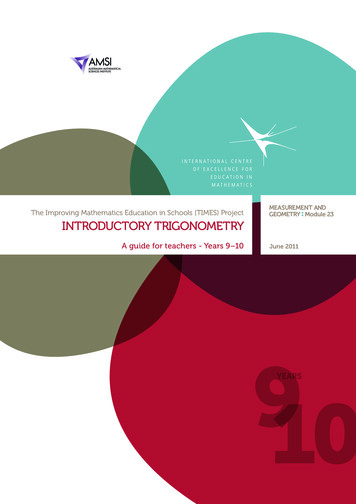
NNU RNs SPONSORNATIONAL RATIOSLEGISLATIONNurse staffing standards for Hospital Patient Safety and Quality Care Act —S. 1357, Senator Sherrod Brown; H.R. 2581, Representative Jan SchakowskyAfter a landmark report was published byUniversity of Pennsylvania researchers validatingthe lifesaving impacts of the California ratioslaw, which demonstrated that if ratios wereimplemented nationally thousands of lives couldbe saved, NNU members across the nation workedwith legislators to write a federal nurse-to-patientratios law. As a result of continued advocacyefforts of our members, each year more legislatorsagree to support this vital legislation.UNIFORM NATIONALPROFESSIONAL STANDARDS1.Patient advocate duty and right2. Minimum, specific, numerical, unitspecific, direct-care, RN-to-patientstaffing ratios for acute-care hospitals»» Additional staff required based onindividual acuity3. Whistle-blower protection4. Prohibition against averaging of ratiosPROPOSED FEDERAL RN-TO-PATIENTSAFE STAFFING RATIOSBased on patient acuity, with the most criticalreceiving one-to-one careOperating RoomTrauma Patient in ERIntensive/Critical CareNeonatal Intensive CarePost-anesthesia RecoveryLabor & Delivery Burn UnitICU Patient in ER Coronary CareAcute Respiratory CareAntepartum Combined L&D andPostpartum Postpartum CoupletsPediatrics ER Step DownTelemetryIntermediate Care NurseryMedical/Surgical PsychiatricOther Specialty CareRehabilitationSkilled Nursing Facility5. Prohibition against mandatory overtime6. Protection for refusal of unsafepatient assignments7. Tough monetary fines for violations ofratios and employee and patient rights8. Registered nurse workforce initiativeWell Baby NurseryDrawing on the lessonsfrom CaliforniaRNs in states throughout the country are activelyworking with CNA/NNOC and NNU to win theirown mandated direct-care, RN-to-patient staffingratios. Building upon the success achieved inCalifornia, RNs across the country includingNew York, Pennsylvania, and Ohio are pursuingmandated nurse-to-patient safe-staffing ratioslegislation in their states.» There can be no compromise on the needfor mandated, minimum, RN staffing ratios.» RNs must take a highly visible, very publiclead in this fight.» The alliance that counts is between RNs,patients, and the public.» RNs must act collectively in support of ratios.“One of the best natural experiments occurredwhen California enacted mandated nurse-topatient ratios. When it was implemented onJan. 1, 2004, the hospitals that were not incompliance to the staffing ratios had to changeon that day and they did. Our research hasshown that staffing did change substantiallyin California hospitals — even in safety nethospitals, which have been very difficult to get tochange on hospital nurse staffing.Almost 15 years later, California still has thebest nursing-staffed hospitals in the country.The state has seen steeper declines in mortalityand improvements in other indicators thanother states.Our findings suggest that registered nursestaffing in California hospitals increasedconsiderably as a consequence of theimplementation of the state’s nurse staffingmandate. We found no evidence that the policyresulted in lower nursing skill mix, including ahigher proportion of licensed vocational nurses.To the contrary, skill mix increased.”— Linda Aiken, PhD, RNDr. Aiken is a professor of nursing, professor of sociology,and director of the Center for Health Outcomes and PolicyResearch at University of Pennsylvania School of Nursing.She is generally considered the nation’s foremost expert onhealth policy as it relates to the nursing workforce.AHRQ (2018). Perspectives on Safety. “In Conversation With .Linda Aiken, PhD, RN”. R. M. W. MD, U.S. Department ofHealth and Human Services.»» Preceptorship and mentorshipdemonstration project56
PAVING THE WAYThe CNA/NNU fight to winfirst-in-the-nation ratios inCaliforniaIt took years of rallies, protests, publichearings, meetings with legislators,and tens of thousands of letters tonewspapers, but California RNs nevergave up until safe, patient ratios werein place in every acute-care hospital.The nurses’ vigilance to protect ratioscontinues to this day.“When ratios came, I was like‘Hallelujah!’ because we wereable to give true patient care.”Fewer patients meansmore time for quality care“One less patient makes a bigdifference. The fewer patientsyou have, the more time youhave to spend with a patient.And if you’re the patient, youwant your nurse to give youall the care you need.”— Shirley Toy, RN, University ofCalifornia Davis Medical Center,Sacramento, California— Paula Lyn, RN, Alta Bates SummitMedical Center, Oakland, California78
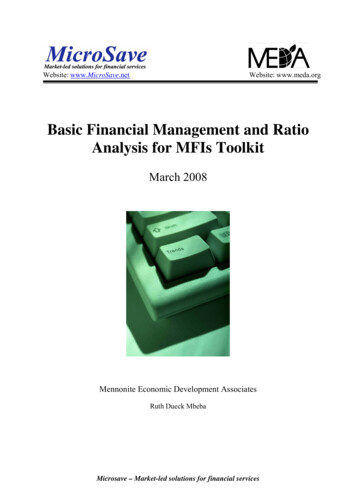
GROUNDBREAKING STUDYON RATIOS SUCCESS STORYLives saved — improved patient carePioneering law on nurses found to save lives“Nurses in California take care of two fewer patients on averagethan nurses in Pennsylvania and New Jersey in general surgery.These differences lead to the prevention of literally thousandsof deaths.”— Linda Aiken, PhD, RN, director of Center for Health Outcomes and PolicyResearch, University of Pennsylvania School of NursingMore nurses, less death“Linda Aiken, who led the studyand directs the Center for HealthOutcomes and Policy Research atPenn, said improved nurse staffinglikely could save ‘many thousands ayear’ nationally.Aiken said the newstudy followed decades of researchshowing that patient outcomeswere better when nurses caredfor fewer patients.”— Philadelphia Inquirer, April 20, 2010A 2010 landmark research project, the mostcomprehensive study done on the California RNstaffing ratios law, proved what California nurseshave long known — California’s ratios are thesingle most effective nursing reform to protectpatients and keep experienced RNs at the bedside.University of Pennsylvania researchers led by LindaAiken, PhD, RN, director of the Center for HealthOutcomes and Policy Research at the Universityof Pennsylvania School of Nursing, interviewed22,000 RNs in California and two comparablestates, Pennsylvania and New Jersey. Theirfindings, published by the policy journal, HealthServices Research, documented that:»» New Jersey hospitals would have 14 percentfewer patient deaths and Pennsylvania11 percent fewer deaths if they matchedCalifornia’s 1:5 ratios in surgical units.»» California RNs have far more time to spendwith patients, and more of their hospitalshave enough RNs on staff to provide qualitypatient care.w-staffing laesrunianCaliforstudy says,sevlisevsa21,Y APRILWEDNESDA2010TUESDAYAPRIL 20,2010y predictsdutsgnNurse staffi ndate wouldmaCaliforniaelsewheresave lives»» Fewer California RNs miss changes in patientconditions because of their workload thanNew Jersey or Pennsylvania RNs.»» In California hospitals with better compliancewith the ratios, RNs cite fewer complaintsfrom patients and families and the nurseshave more confidence that patients canmanage their own care after discharge.20, 2010may aidsitmlidWorkloanursespatients,Y APRILTUESDA»» California RNs are far more likely to stay atthe bedside, and less likely to report burnoutthan nurses in New Jersey or Pennsylvania.910
Q AEverything you everwanted to ask about ratiosQ. Didn’t hospitals make cuts to other staff after the ratioswere implemented?A. No.The number of unlicensed personnel in California hospitals increased by 64 percent from 2005(the first full year the ratios were implemented) to 2011 (the last year that data was available).This compares favorably to the 40 percent increase of unlicensed hospital personnel nationallyover the same period.Q. Have ratios caused an increase in hospital closures?Q. Where will the RNs come from?A. The number of actively licensed RNs in California has increased by nearly130,000 following enactment of the staffing ratios law in 1999.Strong, effective, ratios laws have been a critical factor in helping to mitigate the effects of thenursing shortage. It is well documented that poor nurse work environments create burnout,desire to leave the profession, and high RN turnover rates. After nurse-to-patient ratios were fullyimplemented, nurses returned to the bedside and reported improved job satisfaction.A. No.In 2005, when the hospital industry sought to overturn the ratios law, they failed to produce in courtany evidence linking ratios to hospital closures. Claims by the hospital industry that California’spatient safety law is to blame for hospital and ER closures ignores the fact that 50 hospitalswere closed in California between 1990 and 2000 for market-based reasons, long predating theimplementation of the ratios law.Nationally, 996 hospitals closed from 1987 to 2007, none as a result of California’s safe staffing law.California and the state of Victoria in Australia, both with mandated ratios, prove this point.Q. What if my patients need more care than the minimum ratios?In California, since the signing of the law in 1999:» Vacancies for RNs at Sacramento-area hospitals plummeted 69 percent since early 2004when the ratios were first implemented. Throughout the state, many of California’s biggesthospital systems have seen their turnover and vacancy rates fall below 5 percent, far belowthe national average.A. California’s ratios law sets a floor and is not a “one-size-fits-all”standard. It accounts for additional staffing to meet individualpatients’ needs.— Sacramento Business Journal, January 11, 2008» The number of actively licensed RNs grew by an average of 10,000 a year, compared to under3,000 a year prior to the law’s passage.— California Board of Registered Nursing» There has been a 60 percent increase in RN applications since the law was signed in 1999.— California Board of Registered NursingIt is routine for the industry to respond to patient,nurse, and legislator calls for minimum safe nursestaffing laws with threats of staffing cuts,reduced hiring standards, or cuts to programs.As described above, however, these industrythreats are merely a thinly veiled attemptby hospitals to protect their profits despitethe harm.Victoria, Australia, which adopted nurse-to-patient ratios in 2000:» Experienced a 24.1 percent increase in the number of employed nurses.» There are no vacancies in urban hospitals because better staffing levels lured more than 7,000inactive nurses back into the workforce.1112
High RN turnover is extremely costlyThe average cost of turnover for a bedside RN remains consistent at an average of 49,500 and rangesfrom 38,000 to 85,000. RN turnover will cost a hospital from 4.4– 7 million annually. Each percentchange in RN turnover will cost the average hospital an additional 337,500. Shockingly, despite thetremendous expense of high turnover, 87 percent of hospitals are not tracking the cost of recruiting RNslost to high turnover.Ratios improved RN working conditions, recruitment, and retentionQ. Won’t hospitals just take away all of our support staff? We need them too!A. No.There are specific protections in the law that block the hospital from doing this. The most recentsurvey of nurse employers performed by the University of California San Francisco (UCSF) reportsthat “the share of current staff represented by per diem RNs, LVNs, and unlicensed aides/assistantshas been relatively consistent over the past seven years”. 1Q: What is the link between staffing, better patient outcomes, and decreasedmortality?A: Nurses, who are with patients constantly, understand this link very well.When there are not enough nurses to take care of patients’ needs, care is often missed or leftundone. When lifesaving nursing care is rationed by the hospital, patients suffer more complicationsand preventable death. Missed nursing care is never acceptable. After decades of studies, it is nolonger disputed that ratios save lives. Despite this evidence, hospitals continue to ration nursingcare in understaffed hospitals.Q: Will ratios save hospitals money?A: YES!California’s ratios law demonstrates that compliance with minimum nurse-to-patient staffing laws isundoubtedly feasible, resulting in improved nursing work environments and hospital savings.A comparative study of California to New Jersey and Pennsylvania found that California’s ratios havepositively affected nurses’ overall work environment and their corresponding ability to deliver patientcare. The study went on to find that “[n]urse workloads in Califor nia hospitals in 2006, two years afterthe implementation of mandated nurse staffing ratios, were significantly lower than in New Jersey andPennsylvania hospitals.” 3Combining medical savings with increased productivity, the addition of 133,000 RNs would result in aneconomic value of 57,700 for each of the additional RNs.4Overall, compared to their nurse counterparts in New Jersey and Pennsylvania, nurses in California carefor an average of one fewer patients and reported more favorable outcomes with respect to every workenvironment measure analyzed, including reason able workload, adequate support staff, and enough RNsto provide quality patient care.5After the implementation of California’s ratios law, nurses in California experienced burnoutat significantly lower rates than those in New Jersey and Pennsylvania, and reported less jobdissatisfaction.6 Both burnout and job dissatisfaction are precursors to turnover.A 2009 study estimated that adding 133,000 RNs to the U.S. hospital workforce — the number of RNsneeded to increase nursing staff to the 75th percentile — would produce medical savings of 6.1 billion,not including the value of increased productivity when nurses help patients recover more quickly.7Mandatory, minimum, nurse-to-patient staffing levels are feasible, resulting in better nurse workloads andhospi tal savings from lower turnover rates and dramatically fewer costly complications for our patients.123456713Chu, L.; Spetz, J.; & Bates, T. (July 13, 2017) Survey of Nurse Employers in California, Fall 2016. (p. 31) Retrieved August 14, 2018,from http://bit.ly/CA-NurseEmployersSurvey-2016NSI Nursing Solutions, Inc. (2018) 2018 National Healthcare Retention & RN Staffing Report. Retrieved August 14, 2018,from ntionreport2018.pdfAiken, L. H., et al. (2010) Implications of the California Nurse Staffing Mandate for Other State. Health Services Research, 45(4). (pp. 904-921)Retrieved August 14, 2018, from http://bit.ly/CA-NurseStaffingMandateDall, T. M., Chen, Y. J., Seifert, R. F., Maddox, P. J., & Hogan, P. F. (January 2009) The Economic Value of Professional Nursing. Med Care, 47(1),(pp. 97-104) Retrieved August 14, 2018 from http://bit.ly/EconValueOfProfNursingAiken, L. H., et al. (2010) Implications of the California Nurse Staffing Mandate for Other State. Health Services Research, 45(4). (pp. 904-921)Retrieved August 14, 2018, from http://bit.ly/CA-NurseStaffingMandateibid.Dall, T. M., Chen, Y. J., Seifert, R. F., Maddox, P. J., & Hogan, P. F. (January 2009) The Economic Value of Professional Nursing.Med Care, 47(1), (pp. 97-104) Retrieved August 14, 2018 from http://bit.ly/EconValueOfProfNursing14
THE HALF MEASURESBeware of “staffing” billsmasquerading as ratiosNNU RNs KNOW ONLY THE STRONGESTLANGUAGE WILL PROTECT OUR PATIENTSIn an effort to derail mandated, RN-to-patient,ratios laws, the hospital industry along with itsallies has pushed for passage of inferior “staffing”bills. When analyzing the merits of a particularbill, be suspicious when a bill has any of thefollowing markers.IS IT A REAL RATIOS LAW OR A FAKE,WEAKENED “STAFFING” PLAN?»» Voluntary and/or “permissive” ratios.»» These laws may provide specific, numericratios, however they also include loopholesgiving employers the right to staff as theyplease. One of the loopholes allowsemployers to interchange RNs for“other health care personnel.”»» No public disclosure.»» No enforcement.»» No rights for the RN as patient advocate, nowhistle-blower protection.»» Staffing based solely on patient classificationsystems without ratios as a minimumsafety standard.15These approaches make vague and undefinedreferences to “appropriate” staffing levels withoutproviding specific ratios numbers. Acuity-basedstaffing — using tools developed by hospitalindustry consultants — is presented as analternative to mandated minimum ratios. Allof these “plans” are designed to prevent theimplementation of real, enforceable, RN-to-patientratios that are improved upon per patient need asdetermined by the independent judgment of thedirect-care RN.In states where “staffing plan” style legislation haspassed, there has been little to no change in thenurse-to-patient ratios. In many cases, the hospitalsdo not even create a nurse staffing plan becausethere is no penalty for noncompliance.Nurses must unite and demand nothing short ofminimum, mandated, nurse-to-patient ratios.The industry will continue to push policymakersto adopt toothless reforms. However, nurseshave the power to use our voice as the mosttrusted profession to push for meaningful,lifesaving alterations.Our hospital has added 500 new RNpositions and we rarely use registryor travelers“I work in a medical unit where a majority ofour patients are diabetic and require lots ofteaching and monitoring. Our night-shift RNsused to have nine to 12 patients before theratios were in effect. We could never keepa core nursing staff on nights. As a resultof the ratios law we don’t have morethan five patients, which gives us thetime we need to do patient teachingand has dramatically improved patientoutcomes and nurse retention. Ourhospital has added 500 new RNpositions and we rarely use registryor travelers.”— Mary Bailey, RN, Long Beach MemorialHospital, Long Beach, CaliforniaNNU RNs are able to advocate for the strongestprotections because we have built a powerfulunion run by and for direct-care RNs, not giantcorporations like some other groups who claim torepresent direct-care nurses.16
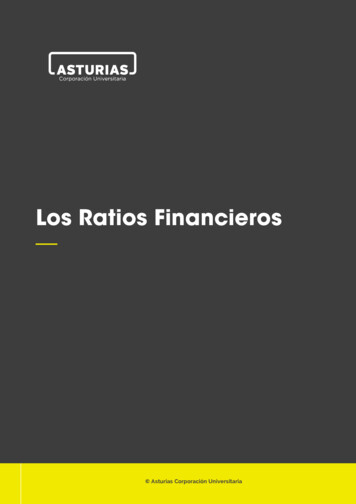
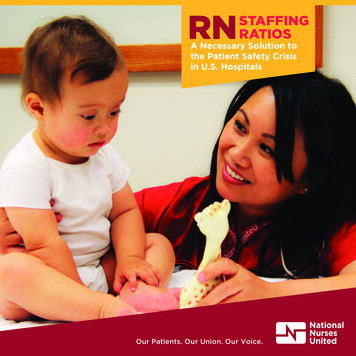
NNU: A NATIONAL SOCIALADVOCACY MOVEMENTFOR RNsA strong voice for ourprofession and our patientsNational Nurses United is a national union andprofessional organization with a powerful agendaof patient advocacy. It is the nation’s largest andfastest-growing union and professional associationof direct-care nurses, tripling in size during thepast 10 years.NNU is recognized by RNs across the nation forour premier, collective bargaining contracts whichenhance the collective voice of RNs in patientcare decisions, outlaw dangerous practices suchas mandatory overtime, dramatically improvesretirement security for RNs, and offers otherprovisions that are needed to retain career RNs atthe hospital bedside and protect patients.NNU is a leading national advocate for universalhealth care reform through a single-payer-stylesystem based on an improved and expandedMedicare for All. The organization is campaigningfor single-payer legislation in Congress; H.R. 1384and S. 1129 (Medicare for All Act of 2019). Nursesbelieve in a single, high-quality standard of care foreveryone. Additionally, we also know that whenour health care system values boosting profits overquality care, the result is compromising patient care— including nurse staffing. A Medicare for All-typesystem places patients first.RN VACANCY ANDTURNOVER RATES BYSTATE AND YEARThis legislation would secure the right to healthcare for everyone and change the values of ourcurrent health care system from corporate valuesto nurses’ values. When nurses’ values drive healthcare decisions, safe staffing, quality nursing care,dignity, and humanity become priorities that arenot sacrificed to boost health care profits.CNA/NNOC and NNU championed to victorythe first-of-its-kind comprehensive workplaceviolence protections in California. This standardhas been heralded by OSHA. Using the momentumfrom that victory, NNU again worked withlegislators to bring those protections to all nursesacross the nation. We are pleased that our federalworkplace violence prevention legislation enjoysbipartisan support.Other landmark laws sponsored by NNU includewhistle-blower protections for caregivers whoexpose unsafe hospital conditions, comprehensiveworkplace violence prevention, a ban oninappropriate personnel providing t elephonemedical advice, and increased funding for nursingeducation programs.For more information, visit our website atwww.NationalNursesUnited.org.A Texas Center for Nursing Workforce study on hospital nurse staffingvacancy and turnover rates for registered nurses showed RN turnoverrates in California to be dramatically lower than states without ratios,such as Florida and Texas(Texas Center for Nursing Workforce Studies, .2%0%Texas 2016Florida 2015California 2015New York 2014Position Vacancy RateMedian Facility Turnover Rate1718
NURSES FROM COAST TOCOAST CAMPAIGN FORSTATE-BASED LEGISLATIONMODELED AFTER THESUCCESS OF THECALIFORNIA LAWCALIFORNIA’S RATIOS LAW SETS A FLOOR AND IS NOT A “ONE-SIZE-FITS-ALL”STANDARD BY ACCOUNTING FOR ADDITIONAL STAFFING TO MEET INDIVIDUALPATIENTS’ NEEDSContrary to the deceptive refrain by industry, laws establishing minimum nurse-to-patient staffing ratiosare just that — baseline on nurse-staffing levels that ensure safe patient care. The ratios law as enactedis akin to other workplace and public health statutes and regulations that set minimum standards toprotect the health and safety of both caregiv ers and the patients they serve. The ratios law demandsmerely what patients deserve — quality care when they seek health care at hospitals.NURSE-TO-PATIENT RATIOS INCREASE NURSE AUTONOMY AND STRESS THEPROFESSIONAL JUDGMENT OF THE DIRECT-CARE REGISTERED NURSENothing in the Califor
the national nursing union it belongs to, National Nurses United, fight to pass ratios laws at both the state and federal level. A seminal 2010 University of Pennsylvania study showed that the California law saves thousands of patient lives, and that if California's 1:5 ratios were matched, surgical units in New Jersey