Transcription
Saudi Journal of Oral and Dental ResearchAbbreviated Key Title: Saudi J Oral Dent ResISSN 2518-1300 (Print) ISSN 2518-1297 (Online)Scholars Middle East Publishers, Dubai, United Arab EmiratesJournal homepage: https://saudijournals.com/sjodrCase ReportOrthodontic Management of Congenitally Missing Lateral Incisor UsingSkeletal Anchorage System – A Case ReportSrinivasan Boovaraghavan*, Ratna Parameswaran, Priyanka Venkatasubramanian, Sanjanaa Venkat, Devaki VijayalakshmiDept of Orthodontics, Meenakshi Ammal Dental College & Hospital Tamil Nadu, IndiaDOI: 10.36348/sjodr.2020.v05i04.006 Received: 14.04.2020 Accepted: 22.04.2020 Published: 27.04.2020*Corresponding author: Srinivasan BoovaraghavanAbstractIntroduction: Congenitally missing maxillary lateral incisor is a most common anomaly that needs to be treatedorthodontically in patients who does not prefer prosthesis. This case report will explain a novel approach to treat theagenesis of maxillary lateral incisor using skeletal anchorage system. Method: 20 years old female patients reported witha chief complaint of spacing and forwardly placed upper front teeth. On diagnosis, Angle s class I dentoalveolarmalocclusion on a class I skeletal base was evident with congenitally missing 12. Patient preferred for space closure of 12regions. Bollard plate was surgically placed on left maxillary tuberosity. 2 TADs were inserted between 14, 15 & 22, 23.Initial alignment of teeth, levelling of bracket slots and space closure in 12 regions were achieved. Brass hooks weresoldered on 0.021" X 0.025" SS arch wire at 2 spots - between 11, 21; 22, 23. E chain was given from bollard plates tohook between 22, 23. Also force was given from TAD placed on left quadrant to the hook soldered between 11, 21 andanother between TAD of the right quadrant to the 2nd molar to achieve complete skewing of the arch and mesialisationof molar on right side to achieve class II molar relation. Result: Angle s class II subdivision dentoalveolar malocclusionon a class I skeletal base was achieved with complete skewing of the dental arch to the left side using skeletal anchoragesystem.Keywords: Orthodontic Congenitally Anchorage dentoalveolar.Copyright @ 2020: This is an open-access article distributed under the terms of the Creative Commons Attribution license which permits unrestricteduse, distribution, and reproduction in any medium for non-commercial use (NonCommercial, or CC-BY-NC) provided the original author and sourceare credited.INTRODUCTIONHypodontia is a dental anomaly, of whichcongenitally missing teeth can be a reason, accountingfor 21.6%. The most common congenitally missingteeth is the maxillary lateral incisor next to the thirdmolar, especially for females.1, 2 The incidence ofbilaterally missing maxillary lateral incisor is twice thanunilateral.3 In unilateral missing cases, the counterparthave a defective in shape and size [4-6]. Missing lateralincisor pose an esthetic problem for the patient if spaceis present in that region. In cases where there isphysiological migration of canine into the lateral incisorspace, aesthetics is less of a concern.The causes for congenitally missing lateralincisor include: (a) Disturbances in the development oftooth, (b) Mild dysplastic expression of ectoderm , (c)Genetics – mutations in genes MSX1, PAX9, TGFA isassociated with congenitally missing tooth, (d)Multifactorial like trauma, cleft lip & palate.[3]status, alveolar ridge morphology, bone support,esthetics, occlusion, gingival margins and availability oflateral incisor space necessitate the need for multidisciplinary approach [7].According to Kokich [8,9,10] treatment forcongenitally missing lateral incisors can be either bysubstitution of canine for laterals or implants and fixedprosthesis in the space of the lateral incisor. Selectingthe treatment modality depends on malocclusion, spacerequirement, tooth size, shape of canine and alsopatient’s preference for prosthetic replacement. Idealtreatment option should be less invasive, conservativeand also esthetically acceptable. Hence caninesubstitution is preferred.This article will explain a conservative methodof orthodontic management in a case of congenitallymissing maxillary lateral incisor.Diagnosis involves both clinical andradiographic examinations. Patient age, periodontal 2020 Published by Scholars Middle East Publishers, Dubai, United Arab Emirates235
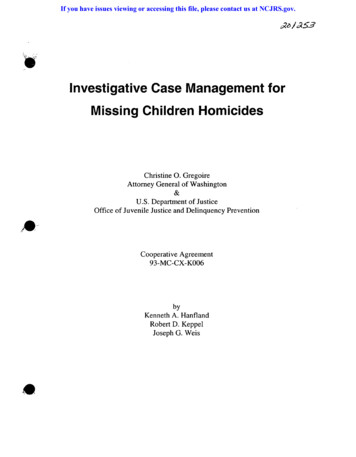
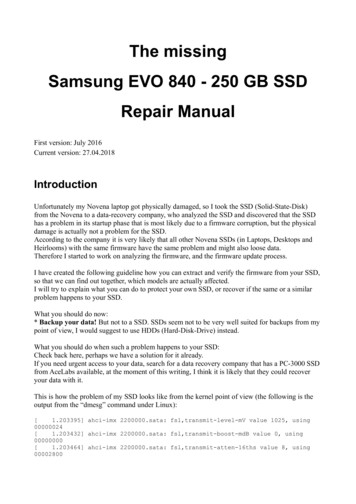
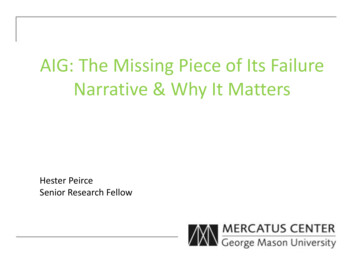
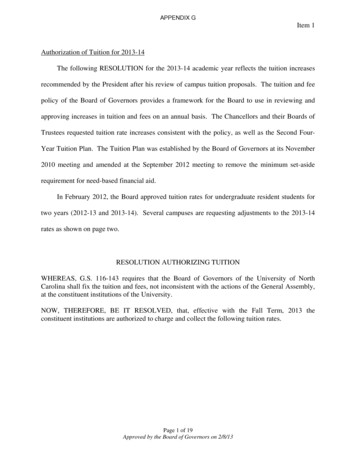
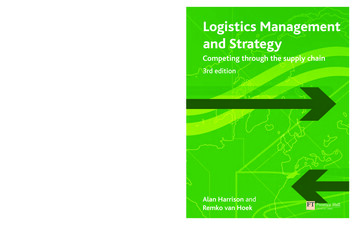
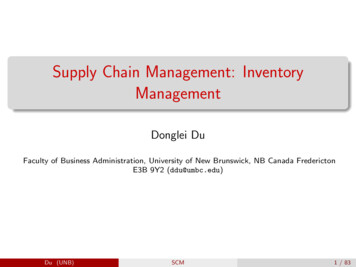
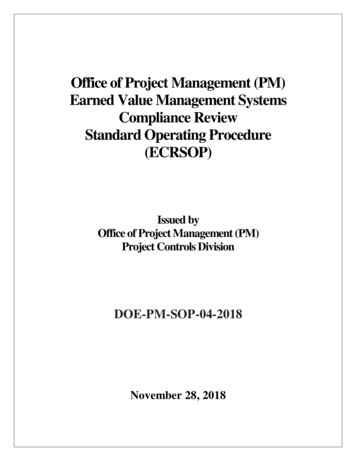
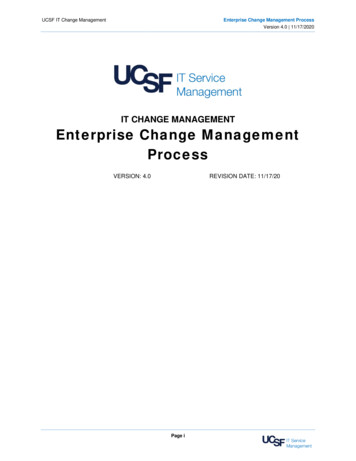
Srinivasan Boovaraghavan et al; Saudi J Oral Dent Res, April, 2020; 5(4): 235-240Diagnosis and treatment planningA 20-year-old female patient working in mediaindustry reported to the department of orthodontics inMeenakshi Ammal dental college with the chiefcomplaint of spacing and forwardly placed upper frontteeth.On frontal extra-oral examination (Fig 1),patient had competent lips at rest. On smile, 80% ofupper incisor and 3mm of lower incisor display wasnoticed with a flat smile arc and spacing in relation to12. The upper dental midline was shifted to right inrespect to the facial midline by 2mm and lower dentalmidline coincided with the facial midline. Whereas onprofile view, she had a mild convex profile with smalldegree of posterior divergence, negative lip step,average nasolabial angle, average mento - labial sulcusand an ideal chin throat angle. On 45-degree obliqueview, she had good cheek bone contour on smile andmild proclination of upper incisors.On intra oral examination, patient had class Icanine and molar relationship bilaterally with missingmaxillary right lateral incisor and edge to edge biterelation. Both the maxillary and mandibular arch wereovoid with mild rotations in premolars.Radiographically (Fig 2), OPG revealedcongenitally missing maxillary right lateral incisor.Cephalometrically, patient had class I skeletal baseattributing to orthognathic maxilla and orthognathicmandible, with an average mandibular plane angle,proclined upper and lower anteriors.Treatment options Maintain class I molar relation on both sides, alignthe arches and prosthetic replacement in relation to12 – implant/ FPD / RPD. Implants / FPD werepreferred for esthetic reasons. Space closure of 12 regions by mesialising upperright quadrant to achieve class II molar relation onright side. Convert canine to lateral incisor and 1 stpremolar to canine by smile designing.Patient did not prefer prosthesis, hence option 2was decided.Treatment progressBollard plates were surgically placed in the leftbuccal region of maxillary tuberosity. Two temporaryanchorage devices – mini screws of 1.3 x 8 mm wereplaced on both the 1st and 2nd quadrant.On the rightside, between the 1st and 2nd premolars and on the leftside, between the lateral incisor and canine at the timeof maxillary teeth strap up. 0.016” NiTi was engaged asthe initial archwire. On the second visit, the lowerposteriors were strapped up and 0.016” NiTi archwirewas engaged. In the maxillary arch, space was closedbetween the 11 & 13 using closed coil spring.At the end of alignment and levelling, therotations were corrected. During the phase of retraction,brass hooks of height equivalent to the level of the TADwere soldered between 11 & 21; 22 & 23 on 0.021“x0.025 “SS arch wire to derive bodily movement. Echain was given from the bollard plates to the solderedhook between 22 & 23 and another E – chain was givenbetween TAD on the left side to soldered hook between11 and 21 (Fig 3). Force was given from right 2 nd molarto the TAD that was placed between 15 & 16. Thishelped in complete movement of the upper archdentition more towards the left side. A prefabricatedarch wire would have caused crossbite on left side andscissor bite on right side as the dental arch skewscompletely. To avoid this, the arch wire was constrictedon the right side and slightly expanded on the left side.Blue bites were bonded on the occlusal surfaces oflower first molars for disocclusion to facilitateasymmetrical arch movement. There was mesialisationof the right upper quadrant, thereby class II molar wasachieved on right side and upper midline shift wascorrected. Care was taken to maintain the class I molaron left side inspite of the unilateral skewing of the arch.Settling elastics were given (Fig 4).The wire sequence used: 0.06 “NiTi, 0.016 “x0.022” NiTi, 0.017” x 0.025” NiTi, 0.019” x 0.025”NiTi, 0.021” x 0.025” NiTi, 0.021” x 0.025” SS.TREATMENT RESULTAfter debonding, digital smile designing wasdone to convert maxillary right canine into maxillaryright lateral incisor and maxillary right 1st premolarinto maxillary right canine. Composite restoration wasdone on maxillary right 1st premolar buccal cusp tip tomimic the canine morphology. Canine was recontouredand reshaped to establish the lateral incisor morphology(Fig 5). Post treatment photographs revealed class Icanine relationship on both side, class I molar on leftside and class II molar on right side with ideal overbiteand overjet.There were no evidences of root resorption(Fig 7). Additionally, Begg’s wrap around retainer wasgiven for the maxillary arch (Fig 6).Post treatment OPG revealed that considerableamount of root parallelism was achieved except inrelation to 15 (Converted 1st premolar). There are noevidences of root resorption (Fig 7).The entire treatment duration was 2 years. 2020 Published by Scholars Middle East Publishers, Dubai, United Arab Emirates236
Srinivasan Boovaraghavan et al; Saudi J Oral Dent Res, April, 2020; 5(4): 235-240Fig-1: Pre - Treatment photographsFig-2: Pre - Treatment RadiographsFig-3: During treatment photographsFig-4: Settling photographs 2020 Published by Scholars Middle East Publishers, Dubai, United Arab Emirates237
Srinivasan Boovaraghavan et al; Saudi J Oral Dent Res, April, 2020; 5(4): 235-240Fig-5: Digital smile designingFig-6: Post - Treatment photographsFig -7: Post - Treatment RadiographsDISCUSSIONThe demand for orthodontic treatment incongenitally missing lateral incisor cases is high whenpatients don’t prefer prosthesis.[11] Esthetics &occlusion must be the deciding factor in the finalpositioning of the anterior teeth. Application of goldenproportion leads to a need for recontouring the caninefor lateral incisor. In patients with unilateral missing oflateral incisor, the esthetics and occlusion are dictatedby the contralateral lateral incisor [12]. In patients withhigh smile line, demand on esthetic result is enhancedas the amount of teeth exposure increases. Unilateral 2020 Published by Scholars Middle East Publishers, Dubai, United Arab Emirates238
Srinivasan Boovaraghavan et al; Saudi J Oral Dent Res, April, 2020; 5(4): 235-240absence of lateral incisor is difficult to manage asachieving the midline symmetry which contributes tothe dental harmony becomes a task [13].Various studies have commented on thegingival esthetics in congenitally missing lateralincisors. Ideal gingival margin of central and canine areexpected to be in the same level when compared withlateral incisor which is 1mm incisal when compared.This poses problem in case of orthodontic space closureand canine substitution [14].This case demonstrates a novel approach for acongenitally unilateral missing lateral incisor usingskeletal anchorage system. The introduction of skeletalanchorage system in the field of orthodontics pavedway for various complicated procedures. Surgicalinsertion of mini – plates is the only concern for thepatients. The force applied from the skeletal anchoragedevice was well established in this case. Skeletalanchorage system was used for rotation of entiremaxillary dentition without tipping.Orthodontists use asymmetrical arch-wires andasymmetrical elastics in correction of asymmetry. It hasbeen reported that adjustments need to be made onarch-wire by skewing it to one side to maintainadequate arch form [15].The benefits of canine substitution areavoiding prosthesis, treatment cost, solving anyprevious crowding. In case of Mesialisation, intrusionof canine and extrusion of first premolar is required inorder to mimic the morphology of lateral incisor andcanine respectively. In case of closure of lateral incisorspace, crown torque of mesially relocated canine shouldbe considered and the duration of treatment can also bemore. The occlusion of patient with Mesialisation ofposterior segment is satisfactory in both esthetic andfunctional point of view [16].Araujo et al. suggests that, in patients withcongenitally missing lateral incisors, if the canine eruptsmore mesially, then canine substitution is the besttreatment of choice. In cases of congenitally missinglateral, where the orthodontic treatment involvesMesialisation of canine, the torque and intrusion ofcanine has to be dealt with. Such method of mesialisingcanine to replace lateral is considered more esthetic andfunctionally considered better. Long term studies haveshowed that there is not much on occlusal overload onthe premolars. However, Bolton s would be of aconcern. There might be mild increased overjet andoverbite, but we were able to achieve ideal overbite andoverjet as there was no discrepancy on the tooth size[17].Paduano et al. suggests that, in average or highmandibular plane angle cases, space closure in theregion of agenesis is preferred, as they preserveanchorage and avoid clockwise rotation of mandible.Also reduced overbite facilitates space closure. Thepresence of 3rd molar also supports for the space closureand Mesialisation of molar on the right side [18].CRITICAL APPRAISALCanines always have a darker shade. Henceconverting canine into lateral incisor will have a mildcompromise in esthetics. Colour matching or bleachingwill enhance the esthetics.As the patient had to leave the city, time wasinsufficient to achieve bodily movement of the 2 ndpremolar. Nevertheless, a good intercuspation wasachieved.REFERENCES1.Uslu, O., Akcam, M. O., Evirgen, S., & Cebeci, I.(2009). Prevalence of dental anomalies in variousmalocclusions. American Journal of Orthodonticsand Dentofacial Orthopedics, 135(3), 328-335.2. Vanarsdall, R. L. (1
Bollard plates were surgically placed in the left buccal region of maxillary tuberosity. Two temporary anchorage devices – mini screws of 1.3 x 8 mm were placed on both the 1st and 2nd quadrant.On the right side, between the 1st and 2nd premolars and on the left side, between the lateral incisor and canine at the time of maxillary teeth strap up. 0.016” NiTi was engaged as the initial .