Transcription
Community-Acquired Pneumonia Clinical Practice GuidelinesPhilippine Clinical Practice GuidelinesDiagnosis, EmpiricManagement and Prevention ofCommunity-Acquired Pneumoniain Immunocompetent Adults2016 UpdateTreatmentI CRMO B I O L O GYANDIPNEPIT IO US DI SEAS O C I ETYFE CINFORJoint Statement ofPSMID PCCP PAFP PCRES970 A D--SPH-- -1-Philippine Copyright 2016IL
2016 UpdateCOMMUNITY-ACQUIRED PNEUMONIAINTRODUCTIONInternationally, community-acquired pneumonia (CAP) remainsthe leading cause of death from an infectious disease. It is the sixthleading cause of death overall and is a major cause of morbidityand mortality. Since the last publication of Philippine ClinicalPractice Guidelines on the Diagnosis, Empiric Management,and Prevention of Community-acquired Pneumonia (CAP) inImmunocompetent Adults in 2010, several changes had emerged: Multiple international societies had published and revisedtheir guidelines of the management of patients with CAP. New organisms had emerged and development of resistancehad increased over time among respiratory pathogens. The influx and efflux of antimicrobial agents used in thetreatment had likewise posed a threat to the rapid riseof antimicrobial resistance. The use, misuse, abuse andoveruse had also shaken the market of antimicrobial agents.It is for these reasons that a long overdue update on themanagement of CAP is needed. There is a need to standardizecare by providing management strategies based on best availableevidences. The evidences may be the same; however, regionaldifferences, causative agents, antibiotic resistance rates, druglicensing, healthcare structure and available resources mayvary. Recommendations made by one national organization maytherefore not be applicable to other countriesTREATMENTWhen should antibiotics be initiated for the empiric treatmentof community-acquired pneumonia (CAP)? Patients should receive initial therapy as soon as possibleafter the diagnosis is established.Antibiotics, the mainstay for the treatment of pneumonia, shouldbe initiated as soon as a diagnosis of CAP is made. The 2004PCPG for CAP recommended a maximum four-hour window1
Community-Acquired Pneumoniafrom diagnosis to antimicrobial initiation. This recommendationwas based on studies that showed a reduced in-hospital mortalitywhen antimicrobial therapy was initiated within the first fourhours of admission and diagnosis of CAP. The 2007 IDSA ATSGuidelines, however, found an internal inconsistency in outcomesbetween the group that received antibiotics within the first twohours and the group which received antibiotics two to four hoursafter diagnosis. Although therapy within 4 hours of arrival tothe hospital has been associated with reduced mortalities insome studies, undue emphasis on early therapy could lead tounnecessary use of antibiotics and associated complications.For these reasons, the present guideline maintains its position tonot recommend a specific time interval between diagnosis andantibiotic administration for patients.Reference:1.Bordon J, et al. Early administration of the firstantimicrobials should be considered a marker of optimalcare of patients with community-acquired pneumoniarather than a predictor of outcomes. InternationalJournal of Infectious Diseases 17 (2013) e293–e298.2.Gattarello S et al. Improvement of antibiotic therapy andICU survival in severe non-pneumococcal communityacquired pneumonia: a matched case–control study.Critical Care (2015) 19:335. doi: 10.1186/s13054-0151051-1.3.Mandell, Lionel A et al. Infectious Diseases Societyof America/American Thoracic Society ConsensusGuidelines on the Management of Community-AcquiredPneumonia in Adults. CID 2007; 44 (Suppl 2): S27-72.4.Philippine Clinical Practice Guidelines on the Diagnosis,Empiric Management, and Prevention of Communityacquired Pneumonia (CAP) in Immunocompetent Adults: 2004 Update.5.Simonetti A, et al. Timing of antibiotic administrationand outcomes of hospitalized patients with communityacquired and healthcare-associated pneumonia. ClinicalMicrobiology and Infection. 2012; 18(11):1149-1155.2
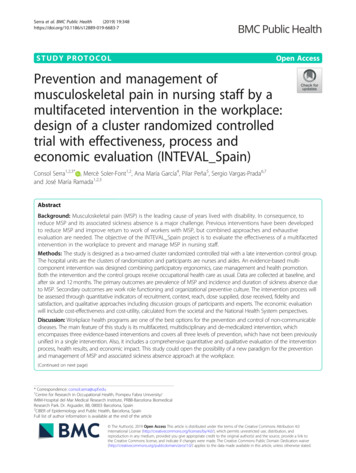
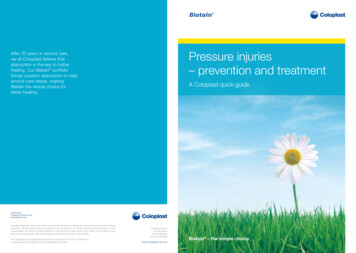
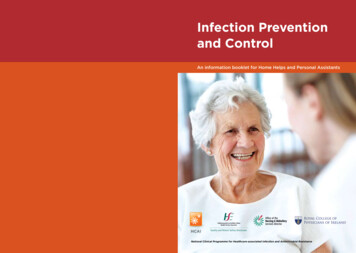
2016 UpdateWhat initial antibiotics are recommended for the empirictreatment of community-acquired pneumonia? For low-risk CAP without comorbid illness,AMOXICILLIN remains the standard drug of choice. Useof extended macrolides may also be considered For low-risk CAP with stable comorbid illness, β-lactamwith β-lactamase inhibitor combinations (BLIC) or secondgeneration cephalosporins with or without extendedmacrolides are recommended. For patients who havecompleted first-line treatment (BLIC or 2nd generationcephalosporin) with no response, an extensive workup should be done to identify the factors for failure ofresponse. Work-up may include doing sputum Gram stainand culture. For moderate-risk CAP, a combination of an IV nonantipseudomonal β-lactam (BLIC, cephalosporin)with either an extended macrolide or a respiratoryfluoroquinolone is recommended as initial antimicrobialtreatment. For high-risk CAP without risk for Pseudomonasaeruginosa, a combination of an IV non-antipseudomonalβ-lactam (BLIC, cephalosporin or carbapenem) witheither an IV extended macrolide or an IV respiratoryfluoroquinolone is recommended as an initial antimicrobialtreatment. For high-risk CAP with risk for P. aeruginosa, acombination of an IV antipneumococcal, antipseudomonalβ-lactam (BLIC, cephalosporin or carbapenem) withan extended macrolide and aminoglycoside OR acombination of an IV antipneumococcal, antipseudomonalβ-lactam (BLIC, cephalosporin or carbapenem) and an IVciprofloxacin or high dose IV levofloxacin.3
Community-Acquired PneumoniaTable 1. Empiric Antimicrobial Therapy for CAPWITH USUAL RECOMMENDED DOSAGES IN 50-60 KGADULTS WITH NORMAL LIVER AND RENAL IRICTHERAPYLow-risk CAPStable Vital signsRR 30/minutePR 125/minSBP 90 mm HgDBP 60 mm HgTemp 36oC or 40oCNo altered mentalstate of acute onsetNo suspectedaspirationNo or stable co-morbidconditionsChest X ray– localized infiltrates- No evidence ofpleural effusionStreptococcus pneumoniaeHaemophilus influenzaeChlamydophila pneumoniaeMycoplasma pneumoniaeMoraxella catarrhalisEnteric Gram-negative bacilli(among those with co-morbidillness)Without co-morbid illnessAmoxicillin 1 gm TIDORExtended macrolidesa:Azithromycin 500 mg ODOR Clarithromycin 500 mgBIDWith stable co-morbid illnessβ-lactam/β-lactamaseinhibitor combination(BLIC)b OR 2nd gen oralcephalosporinc /- extendedmacrolidesaCo-amoxiclav 1 gm BID ORSultamicillin 750 mg BID ORCefuroxime axetil 500 mg BID /Azithromycin 500 mg OD ORClarithromycin 500 mg BIDModerate-risk CAPUnstable Vital Signs:RR 30/minPR 125/minTemp 36oC or 40oCSBP 90 mmHgDBP 60 mmHgAltered mental state ofacute onsetSuspected aspirationUnstable/Decompensatedcomorbid condition-uncontrolled diabetesmellitus,-active malignancies-neurologic disease inevolution,-congestive heart failure(CHF) Class II-IV-unstable coronary arterydiseaseStreptococcus pneumoniaeHaemophilus influenzaeChlamydophila pneumoniaeMycoplasma pneumoniaeMoraxella catarrhalisEnteric Gram-negative bacilliLegionella pneumophilaAnaerobes (among thosewith risk of aspiration)4IV non-antipseudomonalβ-lactamd(BLIC, cephalosporin) extended macrolidesa orrespiratory fluoroquinolonese(PO)Ampicillin-Sulbactam 1.5 gmq6h IV ORCefuroxime 1.5 g q8h IV ORCeftriaxone 2 g OD Azithromycin 500 mg ODPO ORClarithromycin 500 mg BIDPO ORLevofloxacin 500 mg ODPO ORMoxifloxacin 400 mg OD PO
2016 UpdateIf aspiration pneumonia issuspected and, a regimencontaining ampicillinsulbactam and/ormoxifloxacin is used, thereis no need to add anotherantibiotic for additionalanaerobic coverage. Ifanother combination isused may add clindamycinto the regimen to covermicroaerophilic streptococci.-renal failure on dialysis-uncompensated COPD-decompensated liverdiseaseClindamycin 600 mg q8h IVORAmpicillin-Sulbactam 3 gq6h IV ORMoxifloxacin 400 mg OD POHigh-risk CAPAny of the clinical featureof Moderate risk CAPplus any of the following:Severe Sepsis and SepticShock OR Need forMechanical VentilationStreptococcus pneumoniaeHaemophilus influenzaeChlamydophila pneumoniaeMycoplasma pneumoniaeMoraxella catarrhalisEnteric Gram-negative bacilliLegionella pneumophilaAnaerobes (among those withrisk of aspiration)Staphylococcus aureusPseudomonas aeruginosaNo risk for P. aeruginosaIV non-antipseudomonalβ-lactamd IV extended macrolidesaor IV respiratoryfluoroquinoloneseCeftriaxone 2 gm OD ORErtapenem 1 gm OD Azithromycin dihydrate500 mg OD IV ORLevofloxacin 500 mg ODIV ORMoxifloxacin 400 mg OD IVRisk for P. aeruginosaIV antipneumococcalantipseudomonal β-lactamf(BLIC, cephalosporinor carbapenem) IVextended macrolidesa aminoglycosidegPiperacillin-tazobactam4.5 gm q6h ORCefepime 2 gm q8-12h ORMeropenem 1 gm q8h Azithromycin dihydrate500 mg OD IV Gentamicin 3 mg/kg OD ORAmikacin 15 mg/kg ODOR5
Community-Acquired PneumoniaIV antipneumococcalantipseudomonalβ-lactamf (BLIC, cephalosporinor carbapenem) IV ciprofloxacin / high doselevofloxacinPiperacillin-tazobactam4.5 gm q6h ORCefepime 2 gms q8-12h ORMeropenem 1 gm q8h Levofloxacin 750 mg ODIV ORCiprofloxacin 400 mg q8-12hIVIf MRSA pneumonia issuspected, addVancomycin 15 mg/kg q8-12 hORLinezolid 600 mg q12h IVORClindamycin 600 mg q8h IVExtended macrolides: azithromycin, clarithromycinOral β-lactam/β-lactamase inhibitor combination (BLIC) – amoxicillin-clavulanic acid, sultamicillinOral second-generation cephalosporin: cefuroxime axetilIV non-antipseudomonal β-lactam (BLIC, cephalosporin or carbapenem): ampicillin-sulbactam,cefuroxime Na, ceftriaxone, ertapeneme. Respiratory fluoroquinolones: levofloxacin, moxifloxacinf. IV antipneumococcal, antipseudomonal β-lactam (BLIC, cephalosporin or carbapenem):piperacillin-tazobactam, cefepime, imipenem-cilastatin, meropenemg. Aminoglycosides: gentamicin, amikacinabc.d.References:Low Risk CAP:1.Asadi L et al. Guideline adherence and macrolidesreduced mortality in outpatients with pneumonia.Respiratory Medicine (2012) 106, 451-4582.Chalmers JD et al. Increasing outpatient treatment ofmild community-acquired pneumonia: systematic reviewand meta-analysis. Eur Respir J 2011; 37: 858–864.Department of Health. Antimicrobial ResistanceSurveillance Program (ARSP) 2014 Data SummaryReport. Available at 20Report.pdf. Accessedon: 13 June 20153.6
2016 Update4.Laopaiboon M et al . Azithromycin for acute lowerrespiratory tract infections (Review) CochraneDatabase Sys Rev 2015 Mar 8, Issue 3; CD001954. doi:10.1002/14651858.CD001954.pub45.Llor C et al. Efficacy of high doses of oral penicillinversus amoxicillin in the treatment of adults with nonsevere pneumonia attended in the community: studyprotocol for a randomised controlled trial. BMC FamilyPractice 2013, 14:50.6.Pakhale S et al. Antibiotics for community-acquiredpneumonia in adult outpatients. Cochrane Database SystRev 2014 Oct 9;10. CD002109. doi: 10.1002/14651858.CD002109.pub4.7.Petitpretz P et al. Oral Moxifloxacin vs High-DosageAmoxicillin in the Treatment of Mild-to- neumonia in Adults. CHEST 2001; 119:185–195.Moderate Risk CAP:1.Asadi L et al. Macrolide-Based Regimens and Mortalityin Hospitalized Patients With Community-AcquiredPneumonia: A Systematic Review and Meta-analysis.Clinical Infectious Diseases 2012;55(3):371–802.Eliakim-Raz N et al. Empiric antibiotic coverage ofatypical pathogens for community-acquired pneumoniain hospitalized adults (Review) Cochrane Database SystRev 2012, Issue 9:CD004418. doi: 10: 1002/14651858.CD004418.pub43.File TM Jr et al. Integrated analysis of FOCUS 1 andFOCUS 2: randomized, doubled-blinded, multicenterphase 3 trials of the efficacy and safety of ceftarolinefosamil versus ceftriaxone in patients with communityacquired pneumonia. Clin Infect Dis 2010; 51:1395-405.4.Gilbert D et al. The Sanford Guide to AntimicrobialTherapy 44th Edition.5.Kuzman I et al. Efficacy and safety of moxifloxacinin community acquired pneumonia: a prospective,multicenter, observational study (CAPRIVI).BMCPulmonary Medicine 2014, 14:105.7
Community-Acquired Pneumonia6.Lee JH et al. High-dose levofloxacin in communityacquired pneumonia: A randomized, open-label study.Clinical Drug Investigation. 2012; 32(9):569-576.7.Mandell, Lionel A et al. Infectious Diseases Society ofAmerica/American Thoracic Society Consensus Guidelineson the Management of Community-Acquired Pneumoniain Adults. CID 2007;44 (Suppl 2): S27-728.McFarlane A et al. The Value of Macrolide-BasedRegimens for Community-Acquired Pneumonia. CurrInfect Dis Rep. 2015 Dec;17(12):50.9.Mukhae H et al. Efficacy and safety of levofloxacin inpatients with bacterial pneumonia evaluated accordingto the new “Clinical Evaluation Methods for NewAntimicrobial Agents to Treat Respiratory Infections(Second Version). J Infect Chemother 2014 Jul;20(7):41722.10. O brink-Hans K et al. Moxifloxacin PharmacokineticProfile and Efficacy Evaluation in Empiric Treatment ofCommunity-Acquired Pneumonia Antimicrobial Agentsand Chemotherapy April 2015 Volume 59 Number 4:2398-2404.11. Postma DF, et al. Antibiotic Treatment Strategies forCommunity-Acquired Pneumonia in Adults N Engl J Med2015;372:1312-2312. Raz-Pasteur A et al . Fluoroquinolones or macrolides aloneversus combined with β-lactams for adults with communityacquired pneumonia: Systematic review and meta-analysis.Int J Antimicrob Agents 2015 Sep;46(3):242-8.13. Rodrigo C et al. Single versus combination antibiotictherapy in adults hospitalised with community acquiredpneumonia. Thorax 2013 May;68(5):493-5.14. Tamm M et al. Clinical and bacteriological outcomes inhospitalised patients with community-acquired pneumoniatreated with azithromycin plus ceftriaxone, or ceftriaxoneplus clarithromycin or erythromycin: a prospective,randomised, multicentre study. Clinical Microbiology andInfection. 2007; 13(2):162-171.8
2016 Update15.
Community-Acquired Pneumonia from diagnosis to antimicrobial initiation. This recommendation was based on studies that showed a reduced in-hospital mortality when antimicrobial therapy was initiated within the firstfour hours of admission and diagnosis of CAP. The 2007 IDSA ATS Guidelines, however, found an internal inconsistency in outcomes between the group that received antibiotics within .