Transcription
Dr. Poon’sMetabolic Diet“Medication may treatthe number,but weight reductiontreats the cause.”Dr. Pat Poon, Ph.D., M.D.NEWEdition
DR. POON’SMETABOLIC DIETPAT POONB.SC. (HIGHEST HONORS), M.T. (A.S.C.P.,N.C.A.), PH.D., M.D.,AMERICAN BOARD OF PHYSICIAN NUTRITIONSPECIALIST“I can only help those who help themselves.”
The information in this book is true and complete to the best of theauthor's knowledge at the time of publishing. All recommendations aremade without guarantee on the part of the author. The author disclaimsany liability in connection with the use of this information. The authordid not receive any funding from the drug industry in writing this book,and declared no conflict of interest.People with medical conditions and/or taking medications shouldconsult their physicians before starting any diet or exercise program.Do not alter your diet, or change the type or dosage of yourmedications without the approval of your medical professionals.Copyright 2009 by Ontario Nutrition Company Incorporation. Allrights reserved. No part of this publication may be reproduced, storedin a retrieval system, or transmitted in any form or by any means,electronic, mechanical, photocopying, recording or otherwise, withoutprior written permission of the Ontario Nutrition CompanyIncorporation. www.ontarionutrition.caSpecial thanks to Ms. Maria Wong and Ms. Lis Henry for proof readingthe manuscript.Interior Page Composition & Cover Design: Anie Kim ThanPrinted and Bound in CanadaLast digit indicates print number: 12 11 10 9 8ISBN 978-0-9738905-4-9
CONTENTSPREFACEvii1: OBJECTIVES112: WHAT IS OBESITY?153: COMPLICATIONS ASSOCIATED WITH OBESITY23Type 2 Diabetes24Hypertension, Dyslipidemia and Coronary Heart Disease 71Obesity and Cancer87Autoimmune Disease88Acne and Other Skin Disorders89Water Retention91Polycystic Ovary Syndrome92Fatty Liver and Gallstones95Osteoarthritis96Sleep Apnea and Respiratory Problems98Hyperuricemia100Fibromyalgia and Chronic Fatigue Syndrome100
4: CHILDHOOD OBESITY1115: METABOLIC SYNDROME1196: WHY DID THE LOW FAT, LOW PROTEIN,AND HIGH CARBOHYDRATE DIET FAIL?1337: INSULIN IS YOUR ENEMY ANDGLUCAGON IS YOUR FRIEND1398: KETOSIS1459: EAT LOW FAT AND NOT NO FAT15310: MEDICATIONS THAT CAN CAUSE WEIGHT GAIN16311: GLYCEMIC INDEX AND GLYCEMIC LOAD16512: READING FOOD LABELS17313: EXERCISES20714: VITAMINS AND NUTRITIONAL SUPPLEMENTS21715: PROS AND CONS OF DIFFERENT DIETS22516: VITAL STATISTICS23917: PHASE ONE - INDUCTION PHASE24118: PHASE TWO - CONTINUED WEIGHT LOSING PHASE27519: PHASE THREE - MAINTENANCE PHASE29920: FACTS AND MYTHS311
21: “I AM A STRESS EATER”34122: INVASIVE AND NON-INVASIVEBARIATRIC PROCEDURES34723: PHILOSOPHY OF DR. POON’S DIET35124: SUMMARY35525: ABOUT THE AUTHOR359APPENDIX361INDEX371NOTES379
PREFACEIn the animal kingdom, one of the survival skills is the ability to storeexcess food in the form of fat. The animal can use the stored fat as anenergy source when food becomes scarce, for example in thewintertime or in a drought. The human body has maintained thisfeature even after years of evolution as a means of adaptation forsurvival. In this day and age though, food is readily available and thereis no need for us to store fat.One way to determine if you are overweight or obese is to compareyour weight with your height. This is called Body Mass Index (BMI).The United States National Institutes of Health defines “overweight”as a BMI that is over 25 and “obesity” as a BMI that is over 30. By thesecriteria, it is estimated that more than 50% of North America'spopulation is overweight. This definition only applies to the NorthAmerican. It does not apply to the East Asian and Asian. The WorldHealth Organization (WHO) found that, in order to be healthy, the EastAsian and Asian populations need to maintain their BMI at less than 23.A BMI of 23 to 27.5 is considered as overweight for the Asianpopulation. A BMI of greater than 27.5 indicates a high risk for obesityrelated diseases1. Recently the Chinese medical community defined“overweight” in the Chinese population as a BMI that is greater than24.Is obesity a disease? Due to constraints on health care funding, both thegovernment and industry sources do not regard obesity as a disease sothat they do not have to pay for the services. However, you constantlyvii
1: OBJECTIVES* To combat obesity related diseases* To lose fat and excess water weight* To preserve muscle and bone* To lose weight quickly and safely* To keep weight off for lifeWe started this diet program a few years ago to help our patients withmedical problems secondary to their obesity. After a ten-percentreduction in their weight, most of their medical problems became lesssevere, if not totally eliminated. This is particularly true for patientswith metabolic syndrome, Type 2 diabetes, hypertension, indigestion,gastroesophageal reflux, high serum triglycerides, high serumcholesterol, polycystic ovarian syndrome, fluid retention, sleep apnea,arthritis, and fibromyalgia. Surgical patients were frequently referred tous by their surgeons to help them lose weight pre-operatively to lowertheir peri-operative and post-operative morbidity and to decrease thechances of disease recurrence.Metabolism is the set of chemical reactions that occur in livingorganisms in order to maintain life. These processes allow organisms togrow and reproduce, maintain their structures, and respond to theirenvironments. Metabolism is usually divided into two categories:Catabolism and anabolism (Fig. 1). Catabolism breaks down organicmatter for purposes such as harvesting energy in cellular respiration.Anabolism, on the other hand, uses energy to construct components ofcells such as proteins and nucleic acids.11
2: WHAT IS OBESITYRecognized since 1985 as a chronic disease, obesity is the secondleading cause of preventable death, exceeded only by cigarette smoking.Approximately one-third of adults are estimated to be obese.Approximately one in five children in the United States between theages of 6 and 17 are overweight. This number is on the rise.There is a difference between the terms “overweight” and “obesity”.“Overweight” means that there is an excess of total body weight, whichincludes muscle, fat, bone, water, and blood in relation to height.“Obesity”, on the other hand, means that there is an excess of body fatonly. Hence, a body builder may be overweight but not obese, becausehe has a high level of lean body mass. This is why measuring thepatient’s weight alone does not tell the whole story about the patient’sbody composition. Measurement of the body fat percentage is alsoimportant.According to the National Institutes of Health, an increase in bodyweight of 20 percent or more above the desirable weight is the point atwhich excess weight becomes a health hazard.A good way to estimate if someone is overweight or obese is bymeasuring the Body Mass Index (BMI). The Body Mass Index can becalculated using the following formula.15
3: COMPLICATIONSASSOCIATED WITH OBESITYIn this chapter, we will discuss some of the co-morbidities that causedby obesity. There are potential signs and symptoms associated withobesity (Table 1).Table 1. Signs and Symptoms Commonly Found inObese Patients.AppearancesIncrease in size of waistline, neck size, etcThinning of hairIncrease in facial and body hairs in womenWater retention such as swollen feet,hands, and anklesThickened skin fold at the back of the neckand armpitsSkin tags around the neck and armpitsAcneGynecomastia - enlargement of the malebreastWalking with a wide gaitProtrusion of the abdomenStretch marks on skinBuffalo hump below the back of the neckBow legged or knock knees secondary toarthritis of the kneesShortness of breathFatty deposits on upper eyelidsVaricose veinsDiscoloration at the lower limbsSymptomsShortness of breathTiredness, loss of energySomnolencePoor concentration and memoryPainful joints and back, goutHeart burn, indigestion, gallstone attackSnoringSweatingDeep vein thrombosisRapid heart beatsLight-headednessDepression, loss of interestLow self-esteemImpotenceInfertilityIrregular periodRecurrent skin infection, vaginalinfection, cellulitis23
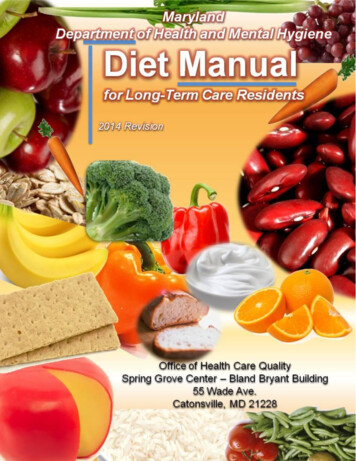
3: COMPLICATIONS ASSOCIATED WITH OBESITYFigure 6. Production of Triglycerides andCholesterol form Glucose.In 2003, the “normal values” of cholesterol, LDL, and HDL have beenreplaced by “target levels”, depending on your risk category ofcoronary artery disease (Table 13). For example, if you belong to thehigh-risk category (Type 2 diabetic, and a patient who has pre-existingcardiovascular disease), your risk of having coronary artery disease inthe next 10 years is more than 20%. Then, in order to avoid a heartattack, your target LDL cholesterol level should be less than 2.5mmol/L, and your Total to HDL cholesterol ratio should be below 4.0.77
4: CHILDHOOD OBESITYWhatever the cause, there is a steady rise in childhood obesity in NorthAmerica. Ten to fifteen percent of the children in U.S. are overweight.Since the gene pool did not change much in the last century, the changein food consumption behavior (increase in consumption of fast foods,soda and juice) by our children is likely the cause of the increasedprevalence of obesity. Due to computer games, television and televisiongames children expend much less energy.One of the most commonly used methods to assess if a child is obeseis to measure the child's BMI. Using the gender specific growth chartsinvented by the United States Centers for Disease Control andPrevention, compare the child's BMI is compared with that of his/herpeers. If the BMI falls between the 85th to 95th percentiles, the child isoverweight. If the BMI is over the 95th percentile, the child is obese.There are risks associated with childhood obesity:1. Social and psychological effects. Overweight children may developlow self-esteem, depression, anxiety, difficulty with relationships,and face discrimination in social situations2. Hypertension3. High cholesterol and triglycerides. Rapid weight gain in the earlyteen years can damage the heart by early adulthood111
5: METABOLIC SYNDROMEAs a teenager, Mr. P was an average height and weight. He participatedin many extra-curricular activities such as soccer, basketball, and martialarts. Even though he ate quite a bit, he did not get fat.While at university, Mr. P worked in the cafeteria and the food was free.He started to overeat. As the workload of his studies got busier, therewas less time for exercise. He began to gain weight.During graduate school, Mr. P stopped overeating and he began toexercise. He was engaged to be married and the wedding was to happenright after he finished graduate school. He wanted to look his best forthe wedding. That was over thirty years ago. Once he got married, hisweight went up steadily. He did not particularly over eat but he wouldeat everything served to him. He did play badminton, but notconsistently enough.His weight was almost 176 pounds (80kg), his waist circumference was103 cm, body mass index was 30 (class 1 obesity), and percentage ofbody fat was 29%. He had headaches and lower back pain. His wife toldhim that he snored loudly. He had hypertension and although he tookthree different antihypertensive medications, his blood pressure was stillhigh (130/95).119
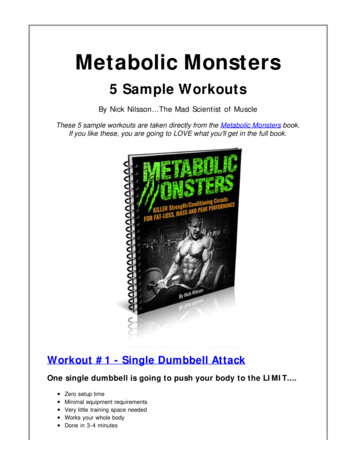
6: WHY DID THE LOW FAT, LOW PROTEIN,AND HIGH CARBOHYDRATE DIET FAIL?You have probably heard this from your friends many times: I work out daily and cannot lose weight I eat only healthy food but I gain weight She can eat so much and stay slim, I starve but still gain weight I am not eating any fat and I eat very little meat. I still cannot loseweightWe want to show you that sometimes it is not how much you eat, but whatyou eat that causes weight gain.In a low-fat low-protein diet, most of your daily caloric intake will haveto come from carbohydrates.133
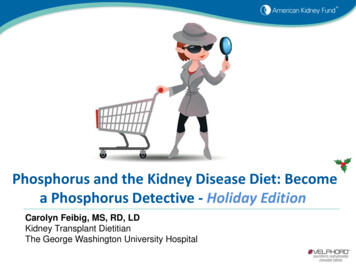
Figure 8. Fat Gain from Eating Carbohydrates.Carbohydrate Intake Fat Build UpEat a piece of breadEatBlood sugar goes up quicklyHungry after 2 hoursInduces InsulinBlood sugar goes downMoves sugar from blood to cellStore extra sugar as FATStore sugar as glycogenIn 1996, researchers showed that subjects who followed a low-fat dietdid not get rid of their obesity, did not lower their cholesterol levels, didlower their HDL levels, and increased their blood level of triglycerideslevel. All the above are risk factors of heart disease.Gram for gram, fat contains more than twice the number of caloriesthan carbohydrates (9 calories vs. 4 calories per gram). Food productsthat contain high amounts of fat are called “energy dense” foods.Cutting back on the amount of total fat in the diet and replacing it withcarbohydrates would seem to be a great way to lose weight. It is easy tounderstand why experts might have first begun recommended a low-fathigh-carbohydrate diet.Cutting back on fat has not worked as well as was first hoped when itcomes to weight loss. While products like low-fat crackers and non-fatcakes have crowded grocery store shelves, we have continued to getfatter and fatter. The reason is, although we are eating less fat, we are134
7: INSULIN IS YOUR ENEMY ANDGLUCAGON IS YOUR FRIENDYou are going to learn how insulin causes obesity and stops you fromutilizing fat as your energy source. It is the objective of this diet toeliminate hyperinsulinemia in order to burn fat. Insulin also increasessalt and water retention (caused by excess secretion of cortisol andaldosterone), that leads to hypertension. Another way insulin causeshypertension is by its involvement in promoting the loss of magnesium.A high insulin level prevents the metabolism of triglycerides andincreases your serum triglycerides level. This eventually causesarteriosclerosis. It has also been implicated in increasing the risk ofType 2 diabetes (by inducing insulin resistance), breast cancer, clottingproblems, colon cancer, gout, sleep apnea, peptic ulcer disease andpolycystic ovarian syndrome.If the doctor injects insu
We started this diet program a few years ago to help our patients with medical problems secondary to their obesity. After a ten-percent reduction in their weight, most of their medical problems became less severe, if not totally eliminated. This is particularly true for patients with metabolic syndrome, Type 2 diabetes, hypertension, indigestion,