Transcription
Social Networks and HealthLisa F. Berkman, Ph.D.Cabot Professor of Public Policy andDirector, Harvard Center for Population andDevelopment StudiesWHOGeneva, June 2-4,2010
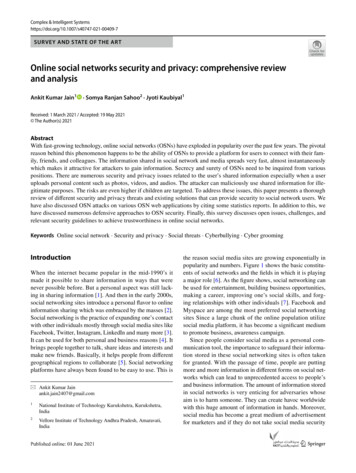
Social Network ModelIND. PersonalCellIntimate IntimateZone A Zone BEffectiveZoneNominalZoneExtendedZoneSource: Bolssevain, Jeremy: Friends of Friends, 1974
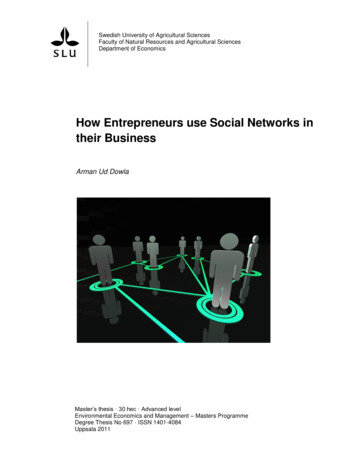
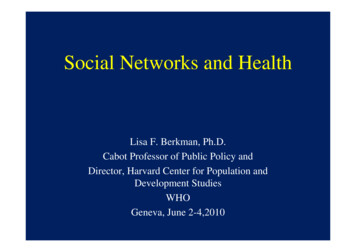
Conceptual Model of How Social Networks Impact HealthUpstream FactorsCondition: the extent,shape, and nature of Social-StructuralConditions (Macro) Socioeconomic FactorsInequalityDiscriminationConflictLabor Market structuresSociogeographic Factors Urban/rural Neighborhood characteristics Residential and occupationalsegregationSocial Change Urbanization War/civil unrest Economic depressionWhich providesopportunities for Social Networks(Mezzo)Culture Language Norms and values Competition/cooperationDownstream Factors Network tyOrganizational structureSocial rankingNetwork Activation Frequency of face-to-faceinteraction Frequency of nonvisual contact Frequency of organizationalparticipation (attendance) Duration and intensity oWhich impacts healththrough the following Behavioral Mechanisms(Micro) Social Support/conflictInstrumental and financialInformational. AppraisalEmotionalConflict/negativeAccess to Resources andMaterial Goods Jobs/economic opportunity Access to health care Housing Human capital Referrals/institutional contactsSocial Engagement Physical/cognitive exercise Reinforcement of meaningfulsocial roles Interpersonal attachmentSocial Influence Constraining/enablinginfluences on health behaviors Attitudes and norms towardhelp-seeking Attitudes and norms towardtreatment adherencePathwaysPsychobiological Pathways Stress-response/allostatic lode Immune system function DHEA levels Glucocoticoid levels Blood pressure Cardiovascular reactivity inflammattion Health BehavioralPathwaysSmoking/alcohol consumptionDietExerciseAdherence to medicaltreatmentsHelp-seeking behavior Psychosocial PathwaysSelf-efficacyCoping effectivenessRelaxation/stress managementDepression/distressSense of well-being/QOL
The upside of social integration,social support:experimentally induced supportor disease exposure
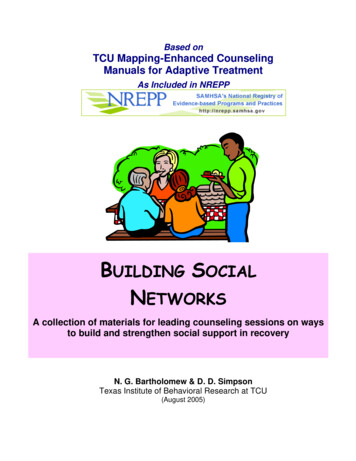
Pittsburgh Common Cold Study N 276:Cohen et al JAMA,1997VIRUS6 Day QuarantineSocial RolesClinical Colds
Social Roles and ColdsCohen et al JAMA,1997O R 4 .2 3 *% with Colds6050O R 1 .8 7 *40O R 1 .0 0301 - 34 - 56 # o f H ig h -C o n ta c t R o le s( O d d s r a tio s a r e a d ju s te d f o r c o n tr o l v a r ia b le s . )
Social Support and Blood Pressure Reactivity toChallenge: experimentally induced blood pressurereactivity
Social Networks and Health:results from observational studies
Social integration and mortalityin a French occupational cohort:EDF-GDF enAdjusted for age, occupational grade, cigarette smoking, alcohol consumption, BMI,depressive symptoms, self-rated health, and geographical region.
Survival curves by marital status andpresence of close confidant1% Survival0.90.80.70.60.5012345Year of Follow-upMarried and/or confidantWilliams et al., JAMA 1992Unmarried, no confidant6
6-Month Mortality post MI byEmotional Support: EPESE100Relative Risk (%)806053%36%4023%20n 53n 111n 260 Sources1 Source2 or More Sources0*P .05.Emotional Support*Source: Berkman, Leo-Summer, Horwitz: Emotional Support and Survival Following Myocardial Infarction. Ann Intern Med, 1992
Caregiving: the upside anddownside
Caregiving in the Nurses HealthStudy.Lee,Colditz,Berkman,Kawachi, AM J Prev Med2003:24(2):113-119 54,412 women in the Nurses Health Study,ages 46-71 (no documented CHD) Information on caregiving in 1992 CHD follow up 1992-1996 321 incident cases, 231 nonfatal, 90 fatal
CHD Risk: Caregivers of Disabled/Ill Spouse3.53.02.52.01.51.00.52978162147100.0Total CHDHours of Caregiving Per Week:Nonfatal CHD01-8 9
Mounting evidence thatcaregiving takes a toll Schulz and Beach. Caregiving strain increasesmortality risk ( RR 1.63) Caregivers have poorer immune function,slower atwould healing( Kiecolt-Glaser et al) Caring for disabled child , telemere length andtelemerase ( Epel, Blackburn et al) Caring for cognitively ill is especiallystressful(EPESE)
Social integration predictsthe preservation of memory inUS elderly:Findings from the Health andRetirement StudyKaren A. ErtelM. Maria GlymourLisa F. Berkman
Methods: Study Sample Health and Retirement Study (HRS) Nationally-representative sample of USresidents born before 1948 4 waves of data collection:– 1998, 2000, 2002, 2004 N 16,638
Methods: Exposure Measure Social integration at baseline (1998)1. Marital status2. Volunteer activities3. Contact with parents4. Contact with children5. Contact with neighborsPossible scores: 0, 1, 2, 3, 4, 5
Results: Trajectory of memory scores comparingsubjects with high versus low social integration10.6Memory score10.4High social integrationLow social YearPredictions are for white males with mean age, income, wealth, and education,and healthiest baseline scores for all health measures.
MIDUS Brief Test of Adult Cognition by Telephone (BTACT)(Lachman & Tun, 2008)TASKTHEORETICAL CONSTRUCT(S) SAMPLE ITEMSWord List Recall(immediate anddelayed)Episodic verbal memory15 words(e.g., flower, truck, school)Backward DigitSpanWorking memorySpans from 2 to 8(e.g., 7, 2, 5, 3 3, 5, 2, 7)Category VerbalFluencyExecutive function, semanticmemoryList as many animals as possible in60 secondsNumber SeriesInductive reasoning5 series of 5 numbers (e.g., 35, 30,25, 20, 15 correct answer 10)BackwardsCountingProcessing speedCounting backward quickly from100AttentionSwitching,Stop and Go TaskSwitchReaction time, attention,task switchingNormal condition:Green Go; Red StopReverse condition:Green Stop; Red GoWith mixed and switched trials
Executive Function &Social Conflict [avg. M1&M2]Age stratified0.5**Means0***-0.5-1-1.532-44(p 0.08)45-54(p .002)Q155-64p 0.03)Q2Q365-74(p 0.32)Q475 (p 0.13)
Can we intervene to promotehealth by improving socialnetworks and social support?
ENRICHD-Enhancing Recovery in coronary heartdisease: ObjectiveBerkman et al: Effects of Treating Depression and Low Perceived Social Support on Clinical Events AfterMyocardial Infarction: ENRICHD Randomized Trial. JAMA, 2003. 289(23) To test the hypothesis that treatment ofdepression and low social support early after anacute myocardial infarction will reduce deathand nonfatal recurrent infarctions.
Study Design ENRICHD JAMA 2003;289:3106 Randomized, parallel-group clinical trial tocompare the efficacy of a psychosocialintervention vs. usual care 2,481 post-MI patients with depression or lowsocial support Average 3.4 years of follow-up Blinded ascertainment of primary endpoint Intention to treat analysis
Baseline to 6-month Changes in SocialSupport and Depression105.15Intervention effectp 0.0010Intervention-5-10-10.1-15ESSIHamilton depressionscoreESSI reported for patients with low social support onlyHamilton depression score reported for depressed patients only
Baseline to 6-month Changes in SocialSupport and Depression105.153.4Intervention effectp 0.0010InterventionUsual care-5-10-8.4-10.1-15ESSI scoreHamilton depressionscoreESSI reported for patients with low social support onlyHamilton depression score reported for depressed patients only
Kaplan-Meier Survival Curves
Social ranking Network Activation Frequency of face-to-face interaction Frequency of nonvisual contact Frequency of organizational participation (attendance) Duration and intensity o Social Support/conflict Instrumental and financial Informational. Appraisal Emotional Conflict/negative Access to Resources and Material Goods Jobs/economic opportunity .File Size: 434KBPage Count: 27People also search fornetworks . comneighborhood support networks for public social support and health older adultsnetworks . com aitela person with type a personalitysocial network in healthacre negative impact