Transcription
McNeely Pediatric Diabetes CenterDiabetes care manualchildrensMN.org
The McNeely Pediatric Diabetes Center islocated on the fourth floor of the Garden ViewMedical Building at Children’s – St. Paul:Address:347 N. Smith Ave.St. Paul, MN 55102Hours: Monday–Friday, 8 a.m. to 4:30 p.m.Phone: 651-220-6624Fax: 651-220-6064Appointments: 651-220-6818Calling the clinicIn a life-threatening emergency, call 911.When calling the clinic, please listen to allof the recorded options before making aselection.Press option 1) to schedule or change anappointment.Press option 2) for all diabetes-related calls,including blood sugar andpump management.Press option 3) for endocrine concerns,including endocrineprescription refills.Press option 4) if your child is ill.If your child has an illness not related todiabetes, please call your primary health careprovider.All diabetes-related callsA diabetes nurse educator will answer alldiabetes calls and return your call as soonas possible. Please leave your name, phonenumber, and child’s full name and date ofbirth, and describe your concern. Calls areanswered regularly throughout the day. Staffwill make every effort to return the call in atimely manner.Ill-child callsPlease leave your name, phone number, andchild’s full name and date of birth. Tell us theproblem and we will make every effort toreturn the call within 30 minutes. If you do notreceive a call back within 30 minutes, pleasecall again.Examples of ill-child calls: Your blood sugar is 80 or less and youcannot eat. Your blood sugar is 300 or higher andyour ketones are moderate or large. You cannot eat or drink for more thanfour hours. You develop dry mouth, cracked lips,sunken eyes, or flushed, dry skin. You have an upset stomach, throw up,have stomach pains, breathe hard andfast, or have trouble staying awake.After-hours callsBefore 8 a.m. and after 4:30 p.m., call651-220-6629 ext. 2, and an answeringservice will take your call and page thepediatric endocrinologist on-call. Youshould receive a call back within 30 minutes.If you do not, ask the service to page thedoctor again. You should always get throughto a person at the answering service. If youdon’t, hang up and call back again.Please reserve this time for urgent calls only,such as those listed above. Do not callafter-hours to review blood sugars, requestpharmacy refills, or ask for appointments.Clinic faxWhen faxing forms to be filled out by clinicstaff, please fill out as much information as youcan yourself. On a cover sheet, tell us where tomail or fax the completed form, and allow fourworking days for us to do the rest.Prescription refillsPlease call your pharmacy for diabetesprescription refills.Pharmacy phone numbers:
Table of contents1.IntroductionWhat to expect from your stay.2About Children’s staff.3Terminology.4,56.HypoglycemiaHypoglycemia . 42Treating hypoglycemia. 43Glucagon. 442.Diabetes basicsWhat is diabetes?.6Understanding type 1 diabetes.7, 8Understanding type 2 diabetes.9Diabetes mellitus complications.107.3.Testing blood sugar and ketonesBlood sugar testing.12Blood sugar control.13All about ketones.14Sick-day guidelinesSick-day guidelines. 46Guidelines for treatment –Basal insulin. 47Vomiting guidelines. 48Exchange list. 49Mini-dose glucagon. 508.ExerciseExercise. 52Insulin adjustments for exercise. 529.Returning to schoolReturning to school. 53, 54Diabetes school supplies checklist. 544.5.Taking insulinInsulin schedules and dosing.16How insulin works.17Basal/bolus insulin regimen.18Storing insulin.19Giving insulin.20Giving insulin shots with syringe.21Insulin pen shot.22Independence in insulinmanagement.23, 24Nutrition and meal planningNutrition and diabetes.26Carbohydrates.27Nutrition labels.28Carbohydrate choices .29, 30Other foods.31Snacks and sweets.32Free foods.33Snack ideas.34Recipe ingredients.35Sugars and sweeteners.36Low carbohydrate product labels.37Food adjustments for exercise.38Tips for healthy eating.39Diabetes and alcohol.40Resources for carb counting andweight management.4110. Coping with diabetesCoping with diabetes. 55Dealing with stress. 56, 57Reaction to stress. 58, 59Development stages andresponses . 60Establishing a routine. 61Responsibility of diabetes care. 62Responsibility of diabetes carecare across the ages. 6211. Diabetes resourceResources at Children’s. 63External resources. 64Financial resources. 6512. Books, magazines and websitesDiabetes books. 66Online resources andmagazines. 67, 68Other resources. 6913. Planning for homeDiabetes skills checklist. 7014. Clinic visit informationDeveloped by the McNeely Pediatric Diabetes Center staff atChildren’s Hospitals and Clinics of Minnesota 2013C31275
Introduction to theDiabetes care manualWe are here to help you and your family!Staff from the McNeely Pediatric Diabetes Center understand the manyquestions and concerns you may have about your recent diagnosis ofdiabetes mellitus. We’ll be here to help, from the first days in the hospital,to your return home, to managing your diabetes every day.This book contains information that will help guide you through yourdiagnosis and management of diabetes. As with any map, it can’t describeeverything that will happen along the way. It can, however, help youprepare for your journey and direct you to resources. These resources canhelp give you more control to support and care for you and your family.Many things are involved in choosing the right diabetes care plan andadjusting it over time. Our goal is to help you achieve the best possiblecontrol with the least lifestyle changes. Our staff will work with you tocombine your knowledge of your child and our knowledge of diabetesto provide the best medical and emotional care possible.This book will be your reference to help you manage diabetes at home.Please be sure to bring this book with you to clinic visits so you can addinformation as you receive it. It also is helpful to have this book availablewhenever you call the clinic with questions. This book is an important partof your diabetes care plan.Throughout the book, “you” most often refers to the person with diabetes.For example, if we say “your doctor,” we mean “your child’s doctor” if youare the parent.There are many things to learn when caring for diabetes. Much of this willget easier as you go along.It’s important that you feel comfortable with everything before you gohome. If you don’t understand something or feel uncomfortable, please talkwith someone on the health care team.We are on this journey together.Children’s Hospitals and Clinics of Minnesota Introduction1
What to expect from your stayYou are in the hospital because you haverecently been diagnosed with Type 1 or Type2 diabetes mellitus. Before you go home, you’lllearn the basic skills of diabetes. You’ll alsomeet many members of your diabetes careteam.The diabetes care team will take you stepby step through learning the basic skills ofdiabetes. These are concepts necessary tolearn and perform before you return home.Whenever possible, all primary caregiversshould learn and perform these skills. It isvery important that primary caregivers bepresent during meals and teaching sessions.Primary caregivers may include parents,grandparents, and day care providers. Duringthis time, please limit visitors so we can focuson your care.Below is an outline of what will take place thefirst few days you are in the hospital. It maychange, depending on your condition andthe needs of your family.Please note, typically education will start at9:30 a.m. each day you are in the hospital.Plan to have all caregivers present and readyby this time for education. This scheduleis always subject to change. Also note, ifanother child is diagnosed with diabetesat the same time, there may be more thanone family present for education. We will,however, make every effort to make sure thatany individual questions or concerns you mayhave are addressed during your hospital stay. Call your insurance provider to talk aboutinsurance coverage. Family begins performing blood sugartests, urine tests, carb counting, andinsulin shots, with help from your nurse. Meet with dietician and possibly meetwith social worker, pharmacist and childlife specialistDay 2 or day of discharge Learn basic skills, including preventionand treatment of low blood sugar(hypoglycemia) with a diabeteseducator. Receive home schedule, schooltreatment authorization form and followup instructions from a diabetes educator. Follow-up appointments. Obtain prescriptions and supplies. Family performs basic skills. Possibly meet with dietician, socialworker, child life specialist, or pharmacist,if this has not yet occurred. Return home.Day 1 Meet with your pediatric endocrinologistto talk about your diagnosis. Learn about diabetes, blood sugartesting, and insulin injection techniquewith a diabetes educator. Your hospital nurse will teach and helpwith menu selections and ketone testing.Children’s Hospitals and Clinics of Minnesota Introduction2
About Children’s staffThere are many pediatric specialists whowill be involved in your diabetes care. Afteryour initial education, you will make a clinicappointment every three months to seea diabetes provider for ongoing diabetesmanagement. We will continue to teach youabout diabetes care at these appointments.You should continue to see your primaryphysician for regular health management.Below are some of the people on yourcare team:Pediatric endocrinologist: An endocrinologistis a physician who specializes in diabetes.Several are on staff at Children’s. One of thesephysicians will supervise your care, both in thehospital and in the outpatient clinic.Pediatric nurse practitioner: The nursepractitioner will usually see your child atthe two-week and six-week follow-upappointments. Many patients see thepediatric endocrinologist and pediatric nursepractitioner at alternate appointments.Dietitian: The registered dietitian will teachyou about diet, its relationship to diabetescontrol, and how to work with yourindividualized meal plan.Pharmacist: The pharmacist will teachyou about insulin and its role in diabetesmanagement.Social worker: The social worker helps familiescope with diabetes by providing emotionalsupport and information about resources atChildren’s and in the community.Child life specialist: A child life specialist willhelp you understand diabetes using ageappropriate language, videos, teaching dolls,books, and more. The specialist also may teachrelaxation and distraction techniques to helpreduce stress or anxiety about needles orother fears.Diabetes educator: The certified diabeteseducator (CDE) will teach you the basic skillsof diabetes management, adjust insulin dosesand provide on-going education. You willlearn about blood sugar monitoring, insulininjections, and preventing and treating lowblood sugars.Children’s Hospitals and Clinics of Minnesota Introduction3
TerminologyAntibodies: Antibodies are produced in thebody as part of the autoimmune process. Theyare responsible for beta-cell destruction.Assessment phase: A period of extra testing(usually 3-5 days) of extra blood sugar checks,at specific times, detailed documentation ofblood glucose, carbohydrate, insulin doses,and activities. The purpose is for gatheringmore data for insulin adjustment or whenstarting a new insulin regime.Beta cells: The small insulin-producing cells inthe pancreas.Bolus: A dose of insulin given for food orcorrection of high blood sugar.Carbohydrates: A component of food. Allcarbohydrates are converted to sugar that isused to provide energy to every part of yourbody. Some people with diabetes need totake insulin when eating carbohydrates.Carbohydrate counting: A process of addingup the carbohydrate content of a meal orsnack. People with diabetes use that total withtheir insulin ratio (dose prescribed by doctor)to calculate the insulin dose.Celiac disease: A condition that damages thelining of the small intestine and prevents it fromabsorbing parts of food that are importantfor staying healthy. The damage is due to areaction to eating gluten, which is found inwheat, barley, rye, and possibly oats.Dehydration: Dehydration happens whenbody fluids are used and not replaced.Increased urination and vomiting can leadto dehydration.Fat: A component of food. Fat does notconvert to sugar when eaten. When fat iseaten with a carbohydrate, it will slow theabsorption of carbohydrates.Free foods: Foods that contain little or nocarbohydrate and can be eaten withoutneeding extra insulin. Examples are lunchmeat, cheese, and vegetables.504 plan: A form that lists the care for a childwith diabetes will need at school.Glucagon: A hormone that raises blood sugar.It is given in the form of an injection for severehypoglycemia.Glucose: What is created when the bodybreaks down carbohydrates for energy. Theterms blood glucose and blood sugar havethe same meaning.Hypoglycemia: Blood sugar that is too low.Hyperglycemia: Blood sugar that is too high.Hemoglobin A1C: A blood test that measuresoverall diabetes control. It is measured everythree months as part of routine diabetes care.Insulin: A hormone, produced in the pancreas,that helps the cells throughout the body usesugar from the bloodstream.Insulin (rapid, such as Apidra , Humalog , andNovoLog ): This type of insulin starts to work in10 to 15 minutes. It works hardest (peak) in 30to 90 minutes and is done working in the bodyin 2 to 3 hours. This type of insulin is designed tocopy the insulin produced by the body whenfood is eaten.Insulin (“peak-less” long-acting, such asLantus or Levemir ): This type of insulin startsto work in four hours. It does not have a peakand is done working in the body in 24 hours.Insulin pump: A small computerized devicethat holds and delivers insulin according toprogrammed or prescribed insulin doses.Individual health plan: A plan written bya school nurse, caregiver, and health careprovider that outlines diabetes caresat school.Insulin resistance: This happens when the bodyis not able to use insulin efficiently.Children’s Hospitals and Clinics of Minnesota Introduction4
TerminologyKetones: Ketones are the by-product of fatbreakdown. When insulin or carbohydrateneeds are not being met, the body breaksdown fat and ketones are produced. Whenketones build up, they spill into the urine. Ahigh level of ketones can cause vomitingand illness.Lancet: The device used to poke the fingerto measure blood sugar.Pancreas: An organ in your body near thestomach. The pancreas has several functions.It produces hormones to help digest food andcontains cells that make insulin.Type 1 diabetes: Also called “juvenile onset”or “insulin-dependent” diabetes. This typeof diabetes is caused by an autoimmuneprocess. The pancreas stops making insulinand insulin injections must be given to treatthis disease.Type 2 diabetes: Also called “adult onset” or“non-insulin-dependent” diabetes. With thistype of diabetes, the pancreas still producesinsulin but the insulin doesn’t work properly.Treatment options may include diet, exercise,medication, and sometimes insulin.Pattern management: A method of lookingat blood sugar readings and the factorsthat affect blood sugar to correctly adjustinsulin doses.Protein: A component of food. Unless eatenin large quantities, protein does not have aneffect on blood sugar readings.Rebound: This happens when high bloodsugar follows a low blood sugar. The highblood sugar is caused by a response in thebody of releasing stored sugar.Syringe: The device used to measure and giveinsulin shots.Target blood sugar range: A goal range whereyour blood sugar should be about 50 percentof the time.Children’s Hospitals and Clinics of Minnesota Introduction5
What is diabetes?Diabetes is a condition in which the bodycannot use the sugar (carbohydrates)from food that is eaten. The body doesn’tmake or properly use a natural hormone,called insulin.When you eat, the carbohydrates in yourfood are broken down into sugar, which yourbody uses for energy. Insulin, a hormonemade in the pancreas (an organ near thestomach), helps the cells throughout thebody absorb sugar from the bloodstream.If you have diabetes, your body cannot usethe sugar, either because it doesn’t makeenough insulin or the insulin it makes doesn’twork right. Since the sugar is not absorbedinto the body, it goes into the urine andleaves the body. The cells of the body arenot able to use the sugar and begin tostarve.Once insulin is given, the blood sugar islowered and the body is able to use thesugar for energy and growth.The two types of diabetesType 1 diabetesType 1 diabetes is also called juvenile-onsetor insulin-dependent diabetes.With Type 1 diabetes: the pancreas stops making insulin. Wedo not know exactly why this happens,but it is an autoimmune process: theimmune system makes a mistake anddestroys the insulin-making cells in thepancreas. insulin must be given to treatthis disease. insulin is a protein; if taken by mouth,it would be digested and thereforenot effective. Therefore, peoplewith Type 1 diabetes require insulininjections each day.Type 2 diabetesType 2 diabetes is also called adult-onset ornon-insulin-dependent diabetes.With Type 2 diabetes: the pancreas produces insulin, but theinsulin doesn’t work properly. treatment options for this type ofdiabetes include diet, medication,and sometimes insulin.Children’s Hospitals and Clinics of Minnesota Diabetes basics6
Understanding type 1 diabetesType 1 diabetes occurs when thepancreas stops making insulin, thehormone that helps thebody absorb sugar from thebloodstream. The other jobsthat the pancreas does, suchas helping digest your food, arenot affected.Figure 2.1Why insulin is neededWithout insulin, the sugar is notabsorbed. Instead, it travelsthrough the bloodstream (whereit can be measured as high bloodsugar), gets filtered by the kidneys,and passes out through the urine.People with type 1 diabetes donot have enough insulin. They willurinate (pee) often, even at night,and are very thirsty. Tirednessand weight loss may also occur,depending on how long the bloodsugar has been high.The warning signs of type 1diabetes are drinking andurinating a lot, weight loss, andlow energy.Causes of type 1 diabetesType 1 diabetes sometimes runs infamilies. However, the majority ofpeople diagnosed have no closerelative with type 1 diabetes. It isnot caused by eating or drinkingtoo much sugar. Sometimes anillness such as a cold or flu canmake the symptoms of diabetesmore obvious. There is nothing anyonecan do to stop Type 1 diabetes fromdeveloping.People with type 1 diabetes developantibodies to the insulin-producing cellsin the pancreas. These antibodies signalthat those cells are being destroyed.We do not know why these antibodiesappear. We do know that replacinginsulin usually produced in the body withinsulin injections will help the body usefood for energy and stay healthy.Children’s Hospitals and Clinics of Minnesota Diabetes basics7
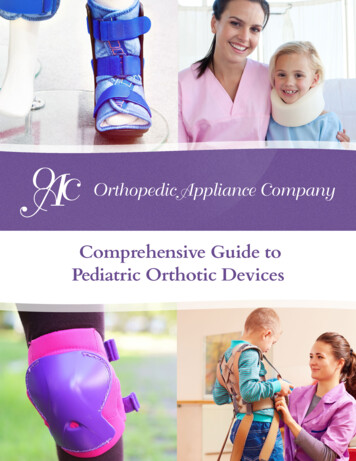
Understanding type 1 diabetesCauses of type 1 diabetesType 1 diabetes develops gradually, overmany months or many years. It does not justcome on suddenly in a week or two beforethe elevated blood sugars.Many insults (represented by arrows in thegraph below) likely result in further damageuntil the diagnoses of diabetes is made. Theinsults may include viral infections, stress,chemicals in the diet, or other agents. Theseagents may work by “activating” antibodiescausing injury and destruction of the insulinproducing cells (beta cells). However, agenetic predisposition (inherited factors)must be present for the process to start.Overtime the beta cells continue to bedamaged until no insulin is produced.Managing type 1 diabetesType 1 diabetes is managed by givinginsulin injections. There are several differentcombinations of long- and short-acting insulinthat the education team will teach you about.All current medical data shows that peoplewith type 1 diabetes will need insulin every dayfor the rest of their lives.For many children, a few weeks after startinginsulin therapy, a “honeymoon” periodbegins. For a short time, the remaining insulinproducing cells (beta cells) in the pancreasmake insulin and a smaller amount of insulinshots will be needed. This can last from afew weeks to one year. There is no test todetermine how long the honeymoon periodwill last.Insulin Production (%)Figure 2.2The gradual onset of type 1 diabetesTime in months or years(Variable for different people)Children’s Hospitals and Clinics of Minnesota Diabetes basics8
Understanding type 2 diabetesPeople who have type 2 diabetes are resistantto the insulin they make. Because the insulinproduced by the pancreas is not workingproperly, the body needs more insulin to helpsugar get into the cells. This type of diabetesis more common in adults. However, peoplewho are overweight or who have other familymembers with type 2 diabetes may develop itat any age.The warning signs of type 2 diabetes are similarto type 1 diabetes since the blood sugar levelsare high in both conditions. People with type2 diabetes drink and urinate a lot and oftenhave weight loss and low energy.Managing type 2 diabetesOften people with type 2 diabetes can controltheir blood sugars with oral medication (pills),exercise, and diet changes. A combinationof these three can help the pancreas makemore insulin and help insulin work better.If the pancreas still cannot keep up with thehigh insulin demands, insulin injections maybe needed. For many children with type 2diabetes, insulin shots are necessary for initialtreatment of high blood sugars.Causes of type 2 diabetesType 2 diabetes runs in families morecommonly than type 1. Also, it is morecommon in certain ethnic groups (AfricanAmerican, Native American, Hispanic, Asian,and Pacific Islander).There are risk factors for type 2 diabetes thatpeople can control unlike type 1 diabetes.These high-risk lifestyle factors include inactivityand a high-fat, high-sugar diet.Make sure you get plenty of exercise (30 to60 minutes every day) and eat foods thatare low in fat and sugar. Avoid concentratedcarbohydrates. (See section 5 “Nutrition andMeal Planning” for more information.)If you have several family members with type2 diabetes or if you had diabetes when youwere pregnant, it is especially important totake control of these lifestyle factors.For people who have type 2 diabetes already,taking control of these lifestyle factors is animportant part of controlling blood sugar anddecreasing complications.Children’s Hospitals and Clinics of Minnesota Diabetes basics9
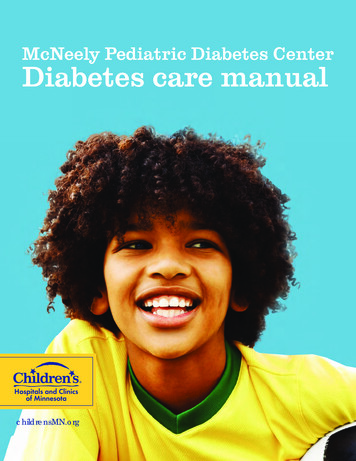
Diabetes mellitus complicationsIf either type 1 or type 2 diabetes is poorlymanaged over several years, complicationscan result. Most are related to somethingcalled microvascular disease.Microvascular disease results when high sugarlevels damage the small blood vessels of thebody. This may cause problems such as retinaldamage (eye problems leading to blindness),kidney problems, heart damage, impotence(sexual dysfunction in men), or nerve damagethat causes numbness of the fingers and toes.Some complications of type 2 diabetes arerelated to high insulin levels needed toovercome the resistance.The test is a marker of overall diabetes control.It is a predictor of long-term complicationssuch as eye disease, kidney disease, andheart disease. People without diabetes haveHbA1C levels less than 6 percent.It is important to set and meet your HbA1Cgoal, because lowering your blood sugarcan reduce your risk of complications, suchas blindness, kidney problems, and heartdamage. The goals for children with diabetesvary based on age and insulin regimen,however they are generally*: younger than 6 years: less than 8.5%,but greater than 7.5 %. 6 to 12 years: less than 8%.Hemoglobin A1COne of the measures of overall diabetescontrol is a blood test called Hemoglobin A1C(HbA1C). The HbA1C test checks averageblood sugar over a three-month period (thelife span of a red blood cell). Your provider willperform this test. older than 12: less than 7.5%.* HbA1C goals based on American Diabetes Associationstandards.Figure 2.3Hemoglobin HbA1CThe chart below shows how Hemoglobin A1C might compare with average blood sugarreadings. Your HbA1C levels should be at the top of the chart to maintain good bloodsugar control.HbA1CAverage bloodsugar **************************360Children’s Hospitals and Clinics of Minnesota Diabetes basics10
Diabetes basics quizCircle T for true or F for false.1. T or FDiabetes is when your body can’t usethe sugar from the food you eat.2. T or FWhen you have diabetes, your pancreasstops making insulin or the insulin it makesdoesn’t work right.3. T or FDiabetes is caused by eating or drinkingtoo much sugar.4. T or FInsulin helps your cells absorb sugarfor energy.5. T or FDiabetes sometimes runs in families.6. T or FDiabetes that is poorly managed (havinghigh blood sugars over several years)can cause complications.Answers: 1. True, 2. True, 3. False, 4. True, 5. True, 6. TrueChildren’s Hospitals and Clinics of Minnesota Diabetes basics11
Blood sugar testingWhen you have diabetes, it is importantto know how much sugar is in your blood.Knowing the sugar level will help you decideon insulin doses and other factors that affectblood sugar.You can find out your blood sugar level bytesting a drop of your blood. You will learnto poke your finger with a lancet device thatwill help you get a drop of blood withouthurting very much.3. Carefully prepare the finger pokerfollowing the manufacturer's directions.4. Poke either side of the fingertip (or toe),not the center or end. Poke in the areabetween the tip and halfway to the firstjoint (no closer to the knuckle than thehalfway point). You can use any finger,but you should use a different fingerevery time.You will test your blood sugar at least fourtimes a day or as directed by your doctor.Testing procedure1. Wash your hands with soap and wateror use an alcohol hand sanitizer. If yourhands are cold, run them under warmwater or shake while hanging yourhands at your sides. This will help to getan adequate blood sample.2. Gather supplies: blood sugar meter5. If the blood does not flow freely, waita few seconds after the poke to let theblood vessels relax. The blood should thenbegin to flow.6. “Milk” the finger gently from the basetowards the tip. Do not squeeze onlyat the fingertip. finger-lancing device (“finger poker”)7. Follow the directions for your blood sugarmeter to correctly check your blood sugar lancets8. Write your blood sugar in your record book. blood sugar testing stripsCongratulations! You did it!Children’s Hospitals and Clinics of Minnesota Testing blood sugar and ketones12
Blood sugar controlWhen to check your blood sugarYou should check your blood sugar beforeeach meal and before going to bed (aminimum of four times daily).For younger children, generally the bedtimeblood sugar should be above 100 mg/dl.Otherwise, blood sugars above 80 mg/dl atbedtime is acceptable.There are certain times when you will needto check the blood sugar more often, suchas when the insulin doses are adjusted, whenassessing current doses, or before clinic visits.This is called an Assessment Phase, whichrequires three to five days of extra checks: before meals three hours after meals, with nocarbohydrates eaten in between mealsIn time, families are encouraged to makeinsulin dose changes on their own, basedon the blood sugar patterns you are seeing.Remember, whenever making insulin dosechanges, it’s important to be checking theblood sugars more frequently. All diabetescenter families are asked to attend the BloodSugar Pattern Management Class in themonths following diagnosis. This class discussesin-depth how to recognize patterns and howto make appropriate insulin dose changes onyour own.Blood sugar control is important in long-termdiabetes management. Research has shownthat improved blood sugar control reducesthe risk for complications of diabetes. Bloodsugar in people without diabetes is between60 and 120 mg/dl. Your doctor will determinethe right target range for you. before bedtimeTarget blood sugar ranges at 3 a.m. for 1-2 nightsExamples of target ranges by age are listedbelow. Your range may be individualizedby your doctor. R
Phone: 651-220-6624 Fax: 651-220-6064 Appointments: 651-220-6818 Call